Compartir en las Redes !
Texit: ¿Es posible la secesión de Texas?
-
verdinegro

- Mensajes: 15294
- Registrado: Sab Dic 18, 2021 10:30 am
- Ubicación: Evropa
- Contactar:
Texit: ¿Es posible la secesión de Texas?
How Greg Abbott's Border Fight Bolsters Calls for an Independent Texas
https://www.newsweek.com/2024/02/09/tex ... 63224.html
The Supreme Court decision to allow federal officials to remove parts of a razor-wire barrier Texas had erected along the border with Mexico—a case of D.C. overruling Governor Greg Abbott—has sparked further calls for the Lone Star State to declare independence from the United States, in a movement called Texit.
"Texas' razor wire is an effective deterrent to the illegal crossings Biden encourages. I will continue to defend Texas' constitutional authority to secure the border and prevent the Biden admin from destroying our property," said Abbott. The concertina wire was installed on his order as a key part of his effort to control illegal immigration.
The de facto leader of the Texit movement, Daniel Miller, remembers as though it were yesterday when he concluded Texas should leave the United States: Saturday, August 24, 1996, at approximately 2 p.m., in the hall of a hotel in the eastern Texan city of Tyler. Such was the impact of that moment that the technology consultant compares it to the "line in the sand" that lore recalls was drawn by his fellow Texan, William Travis, at the Alamo, shortly before it was stormed by Mexican troops in 1836. That legendary siege led to the Republic of Texas, an independent state for nine years before joining the American Union in 1845. Miller, now 50 and the president of the Texas Nationalist Movement (TNM), is hoping to reverse that transition.
Yet despite increased support, the movement has faced several recent setbacks, not least failing to get a referendum vote on Texan secession on the upcoming Republican primary ballot. Critics have also labeled the independence crusade a fantasy that has no chance of success, at least peacefully. But this has not deterred Miller, who remains convinced of his campaign's eventual success.
Miller said: "I think the trajectory the federal government is on, the trajectory that Texas is on, I think we are headed in that direction so whether by conscious decision or collapse of the federal system in its inability to meet its basic requirements, I think Texas becomes an independent nation definitely inside of 30 years."
Fight for a Referendum
By any measure Texan nationalists have had a busy couple of years. In December the TNM delivered what it claimed was a 139,456-strong petition to the Republican Party of Texas in Austin. This called for an advisory referendum on Texan independence to be included on the March 2024 primary ballot.
According to the Texas election code, the minimum number of signatures needed for a referendum to be considered is "five percent of the total vote received by all candidates for governor in the party's most recent gubernatorial general primary election." The most recent Republican gubernatorial primary was in 2022, when 1,954,172 votes were cast, electing incumbent State Governor Greg Abbott. A total of 97,709 signatures are therefore needed for a referendum to be considered. However, the Texas GOP rejected the petition, with chair Matt Rinaldi claiming it had been submitted late, and that even if this hadn't been the case, "the vast majority of petition signatures were invalid." Specifically, he claimed many lacked crucial information such as "the residence address, county of registration, and date of birth/voter registration number" or had been signed electronically, rather than by hand.
This sparked a furious response from Texan nationalists, with Miller announcing on his Texas News podcast that his group was "going to war with the Texas GOP." On January 10, the TNM filed an emergency petition to the state Supreme Court vowing to "fight for your right of self-government," though this was rejected almost immediately.
Texas secessionists have also taken the legislative route, with then-State Representative Bryan Slaton in March 2023 introducing a bill calling for a referendum on "whether or not the State should investigate the possibility of Texas independence," though it failed to pass the legislature's state affairs committee. It came after the Republican Party of Texas approved calls for a referendum on whether the state "should reassert its status as an independent nation" at its June 2022 convention in Houston.
These moves have sparked growing interest in what would happen if Texas did vote to become an independent republic again. In an interview with Newsweek, TNM's Miller argued Texit is the antidote to a failing federal system.
Miller said: "The federal system is broken and Texans are paying the price. It makes more sense for Texans to govern Texas." He blamed the federal government for the rising price of gas and groceries, along with the increasing national debt, adding: "If it could be fixed, it would have been fixed."
What an Independent Texas Looks Like
Miller envisages a successful independence referendum leading to a process of negotiation between Austin and Washington, ending with two independent but closely linked countries. He said: "Once the vote comes back in the affirmative, nothing changes immediately. Texans will begin a process to move toward independence that involves changes to our state constitution, statutes that follow the constitutional changes, evaluation and execution of international covenants, treaties, and agreements and the negotiation of issues with the federal government.
"If the federal government follows its near-centurylong policy of respect for the right of self-determination, we would expect the relationship with the remaining United States to be cordial and cooperative."
On its website the TNM argues an independent Texas should initially continue using the U.S. dollar to provide "economic stability," meaning interest rates would continue to be controlled by the Federal Reserve. In the longer term they call for Texas to seek "a negotiated currency union with the United States," similar to the euro, which is the currency of 20 European countries. If this isn't on offer, "Texas will want to explore moving toward a currency of its own as soon as possible."
Miller told Newsweek Texas would have "no obligation to pay a portion of the debt accumulated by the federal system" and suggested that whether an independent Texas accepts a share would depend on negotiations with Washington over current government assets, including what it would receive from the U.S. military. The TNM claims that after independence Texas would be ruled as a "unitary nation-state," than be subdivided into smaller provinces. Citizenship requirements would be determined by the Texas legislature but "will likely mirror many of the requirements to be a citizen of any other self-governing independent nation," while "Texans who are already legally living within the state when it becomes independent will automatically gain Texas citizenship."
The TNM program also calls for the establishment of an independent Texan military.
According to Miller, the TNM wants "the United States and Texas to maintain a frictionless movement of people and goods between the two" should they split. On its website, the group points to the U.S. relationship with Mexico as a model and states Texas would "readily qualify" for America's federal Visa Waiver program, which allows citizens from 41 countries to enter the U.S. for 90 days without requiring a visa.
Tensions surged in January between Texan and federal authorities over immigration, with Governor Greg Abbott blocking Customs Border and Protection (CBP) officials from patrolling Shelby Park in Eagle Pass, a hotspot on crossings from Mexico.
On January 12 a woman and two children drowned while trying to cross the Rio Grande River opposite Eagle Pass. Two days later, the Department of Homeland Security sent a cease-and-desist letter to Texas Attorney General Ken Paxton giving state authorities until January 17 to allow federal access to the site, or face possible legal action. In response, Paxton refused to back down, with his office vowing: "Texas will not surrender to Biden's destructive open-border policies."
The Battle to Break Free
Any bid at secession would almost certainly result in intense legal disputes, with the Supreme Court ruling in the 1869 Texas v. White case that a state leaving the union is unconstitutional. Miller disputes this view, saying: "Article 1 Section 10 of the U.S. Constitution lists all actions that are prohibited to the states. Withdrawing is not in that list. Therefore, under the 10th Amendment to the Constitution, the lack of an explicit constitutional prohibition means it is a right reserved to the states and the people."
Professor Matt Qvortrup, a political scientist and lawyer, told Newsweek that Texas v. White "is based on somewhat shoddy jurisprudence" and could be overturned by the Supreme Court.
The British academic, author of the 2022 book I Want to Break Free: A Practical Guide to Making a New Country, has studied independence movements across the globe and interacted extensively with Texan nationalists, including addressing the TNM's TEXITCON three-day conference in Waco last November.
During an interview with Newsweek about Texan nationalists, Qvortrup admitted he'd initially "sort of written them off as being on the far right." However, he was pleasantly surprised when a man at an event in Dallas who asked the native Londoner whether he was "terrified to live in a city that is run by a Muslim" was shown the door.
Asked about the Texan secessionist campaigners' chances, Qvortrup said the Lone Star state is "probably the only place in America that has that sense of identity" typically associated with an independent state. For a referendum to take place, the academic argued there would need to be "a political change probably within the Republican Party," followed by a legal battle that could well end up in the Supreme Court. Qvortrup admitted this would be very tough, but added: "100 years ago I think there were about 35 countries in the world. Now it's 195. It's actually not completely impossible to see how countries could establish themselves."
Notably, a number of prominent Texan Republicans have toyed with, if not outright endorsed, secession from the Union. Chip Roy may not have a reputation for mincing his words, but even by the House Republican's standards his statement on January 2 was extraordinary. The United States, he argued, had entered "a constitutional crisis" with central authorities either unable, or unwilling, to "defend our borders from invasion." He added: "My fellow Texans rightly ask whether Texas and similarly minded Americans should remain part of a federal government forsaking their well-being, safety, and security in violation of the compact under which we entered the union."
When asked about Texan independence in November 2021, Senator Ted Cruz said he's "not ready to give up on America yet," but "if the Democrats end the filibuster, if they fundamentally destroy the country, if they pack the Supreme Court, if they make D.C. a state, if they federalize elections, if they massively expand voter fraud, there may come a point where it's hopeless." Should this happen, "then I think we take NASA, we take the military, we take the oil," he said.
'Divorced From Reality'
However, James Henson, director of the Texas Politics Project at the University of Texas at Austin, argued that the debate over Texan independence is more about internal Republican politics than a serious project in its own right.
He told Newsweek: "Texas nationalists calling for something akin to a Texit represent some combination of fantasy and symbolic gesture, each divorced from reality...The GOP party apparatus has become the favored dwelling place of extreme and esoteric elements, where such factions are treated much more seriously than they are among the general public.
"In some areas, they sometimes succeed in moving the center of the party to the right, and in attracting attention to ideas and proposals that have little relation to reality—like the idea of an independent Texas."
Miller bitterly contests the suggestion that Texan nationalism is a right-wing cause, arguing: "For independence movements to be successful they must be trans-partisan in nature." Before co-founding the TNM in 2005, he spent two years studying secessionist movements worldwide, including those in Scotland, Catalonia and Quebec. He attributes Scotland's vote to remain part of the United Kingdom—by 55 percent of the vote to 45 percent—to independence being intertwined with the left-leaning Scottish National Party, and he believes secessionists must "really cut across all those normal ways that politics seeks to divide us" to succeed.
'There Is No Plausible Scenario'
Joshua Blank, an expert in state politics at the University of Texas at Austin, and research director of the Texas Politics Project, argued any Texit is unlikely to be peaceful and would require a greatly expanded state capacity of the type that would repel many Republicans. In an interview with Newsweek, he said: "I think history has made clear that there is no plausible scenario in which Texas could peacefully extract itself from the United States, even were that the will of its populous—which there is no indication of to my knowledge."
Blank continued: "When you start to think about the mechanics of Texas withdrawing from the United States, the ridiculousness of the proposition quickly makes itself apparent. As much as Texas prides itself on the notion of independence, like most states, Texas relies on federal dollars—especially in recent years—to help provide a relatively low baseline of state services. For Texas to withdraw from the U.S., the state would have to significantly increase its revenue through both taxes and fees to make up for lost federal dollars, but also, to begin providing funding for the many, often very expensive, services no longer provided by the federal government.
"A central element of Republican orthodoxy in Texas is a government model based on low taxes and few services. Filling in the gaping financial and service-providing role of the federal government would require a dramatically different, significantly expanded model of government in Texas, one that I would suspect most GOP voters would detest more than Texas' ongoing participation in the United States."
The debate over Texan independence comes amid a broader discussion about the unity, and indeed viability, of the U.S. in the face of current political tensions. In February 2023, House Republican Marjorie Taylor Greene sparked a fiery discussion by calling for a "national divorce" which would see the country "separate by red states and blue states and shrink the federal government."
A subsequent YouGov/Economist poll found 23 percent of Americans agreed with the proposal, versus 62 percent who disagreed and 15 percent who were unsure.
After the Colorado Supreme Court in December ruled Donald Trump constitutionally ineligible to serve a second term as president, due to 14th Amendment restrictions on those engaged in "insurrection," Greene repeated her call on X, formerly Twitter.
The Georgia Republican wrote: "America is in a constitutional crisis. The admin is enabling a full scale border invasion and harboring illegal migrants. The courts are engaging in judicial tyranny. The government is politically weaponized against the people. Soon national divorce may be our only option."
Miller told Newsweek it was "helpful" that Greene sparked the discussion but rejected the idea that the U.S. can be divided between Democrats and Republicans. He said: "This is a union of 50 sovereign states...There is no dividing the United States by political affiliation. It's up to each individual state to determine whether or not they want to continue in this relationship because it is ultimately a voluntary union."
Any effort to divide the United States between Democrats and Republicans would have to contend with the fact there is no obvious geographical split, with conservative-leaning states also containing more liberal pockets, usually around the main cities, and vice versa for some rural areas in Democratic-controlled states.
Growth in Freedom Movements
But this hasn't stopped any number of secessionist movements from laying out their case, particularly when there is geographically concentrated anger over national political events. In the aftermath of Trump's November 2016 election victory, Calexit—like Texit, a play on the term Brexit, used to describe Britain's June 2016 vote to leave the European Union—became a trending topic on Twitter.
A subsequent poll from the University of California, Berkeley's Institute of Governmental Studies found 44 percent of Democrats in the state would support a "proposed statewide ballot initiative that calls for California to declare its independence from the United States and become a separate country," a position held by 32 percent of Californians as a whole.
Carla Gericke is acting president of the Foundation for New Hampshire Independence and a spokesperson for the Free State Project (FSP), a movement which encourages libertarian-leaning individuals to "move to New Hampshire for liberty."
To join the FSP, which it claims more than 20,000 people have already done, individuals are required to "state my solemn intent to move to the State of New Hampshire" then "exert the fullest practical effort toward the creation of a society in which the maximum role of civil government is the protection of individuals' life, liberty and property."
Justifying the policy, the FSP states: "By concentrating our numbers in a single state, we are maximizing our impact as activists, entrepreneurs, community builders, and thought leaders." While not all FSP activists support outright independence for the Granite State, Gericke certainly does, telling Newsweek: "It's an idea whose time has come and a reflection of the frustration everyone on the political spectrum is feeling."
On January 3, Representative Jason Gerhard, a Republican in the New Hampshire legislature, introduced a bill stating that should the federal debt ever reach $40 trillion, around $6 trillion more than at present, the state "shall declare independence and proceed as a sovereign nation."
An apocalyptic take on secession is offered by the upcoming Alex Garland movie Civil War, starring Kirsten Dunst and Nick Offerman, the trailer for which dropped in December. In this play on America's intense political divides, 19 states have left the union, forming factions such as Florida Alliance and what Offerman's three-term U.S. president improbably calls the "so-called Western forces of Texas and California," sparking open war with the American military.
In one clip, militants hold a group of journalists and civilians at gunpoint, one of whom says: "We're American, OK?" One of the armed men, played by Dunst's real-life husband Jesse Plemons, asks: "OK, but what kind of American are you?"
If tensions turn to crisis there are plenty of factions, including Texan nationalists, ready to transform the political geography of North America. The great irony may be that the only force strong enough to bring down the United States, surely the most potent political entity in human history, is itself. As for Miller, when asked about the probability that Texas will be an independent state in 30 years, he didn't show a flicker of doubt. The campaigner simply replied: "100 percent."
-
verdinegro
- Mensajes: 15294
- Registrado: Sab Dic 18, 2021 10:30 am
- Ubicación: Evropa
- Contactar:

Re: Texit: ¿Es posible la secesión de Texas?
En las próximas elecciones veremos que es USA, si ya una nación contaminada por el multiculturalismo, y deja de ser la "Tierra de las Oportunidades", a convertirse en la tierra de los OPORTUNISTAS.
Ahora con esta parada en 4 patas de 5 Gobernadores, a los que seguro se sumaran más gente veremos si los Indígenas Autóctonos que tanto velan por proteger sus territorios y los realmente MADE IN USA, hacen del slogan de Reagan "Let's Make America Great Again" y sacan su PATRIOTISMO, así como se ve en las peliculas de Hollywood, porque...hasta ahora...parece que es eso...pura película, cuando se trata de defender la soberanía de su país y del crecimiento de esta rancia arremetida progre de la que tanto se han cuidado...
Si llegan a ganar los Demócratas en diciembre...el futuro del "mundo libre" está bien negro...y no por el cambio climático...
Ahora con esta parada en 4 patas de 5 Gobernadores, a los que seguro se sumaran más gente veremos si los Indígenas Autóctonos que tanto velan por proteger sus territorios y los realmente MADE IN USA, hacen del slogan de Reagan "Let's Make America Great Again" y sacan su PATRIOTISMO, así como se ve en las peliculas de Hollywood, porque...hasta ahora...parece que es eso...pura película, cuando se trata de defender la soberanía de su país y del crecimiento de esta rancia arremetida progre de la que tanto se han cuidado...
Si llegan a ganar los Demócratas en diciembre...el futuro del "mundo libre" está bien negro...y no por el cambio climático...
Si quieres lograr la perfección, se los mas imperfecto que puedas...
Re: Texit: ¿Es posible la secesión de Texas?
El problema es que el Presidente es el "Commander in Chief" y la mitad de los soldados son panchitos y ahora tienen generales que usan falda porque son hombres que se perciben mujeres.
Veremos si se les siguen uniendo Estados y los John Weyne se aprietan los pantalones.
No es la primera vez que están en salsa. Ya lo vimos en la època de los hippies y el anti americanismo pro Vietnam. Al final se salvaron aunque se perdieron por lo menos dos generaciones entre las comunas hippies y las drogas que usaron para destruir desde dentro la sociedad. Ahora están los progres con sus colectivos LGTVCX FGGHJJk, BLM y Antifa el Cristal Med y el fentanilo sin olvidarnos del antisemitismo.
Yo por los momentos sigo viendo Yellowstone, vamos a ver si esos gringos de verdad existen.
Veremos si se les siguen uniendo Estados y los John Weyne se aprietan los pantalones.
No es la primera vez que están en salsa. Ya lo vimos en la època de los hippies y el anti americanismo pro Vietnam. Al final se salvaron aunque se perdieron por lo menos dos generaciones entre las comunas hippies y las drogas que usaron para destruir desde dentro la sociedad. Ahora están los progres con sus colectivos LGTVCX FGGHJJk, BLM y Antifa el Cristal Med y el fentanilo sin olvidarnos del antisemitismo.
Yo por los momentos sigo viendo Yellowstone, vamos a ver si esos gringos de verdad existen.
-
Senderos

- Mensajes: 8853
- Registrado: Dom Dic 12, 2021 3:59 pm
- Ubicación: https://www.mossad.gov.il/
- Contactar:
Re: Texit: ¿Es posible la secesión de Texas?
Aun faltan gobernadores por sumarse.
Jews Are The Only Indigenous of The Ancestral Land of Israel
Re: Texit: ¿Es posible la secesión de Texas?
Coñoooo, diste en el clavo...con lo de la serie Yellowstone...pensé en ponerlo cuando me referí a Hollywood pero imagine que no se entendería la analogía...Quinoa escribió: ↑Jue Ene 25, 2024 8:07 am El problema es que el Presidente es el "Commander in Chief" y la mitad de los soldados son panchitos y ahora tienen generales que usan falda porque son hombres que se perciben mujeres.
Veremos si se les siguen uniendo Estados y los John Weyne se aprietan los pantalones.
No es la primera vez que están en salsa. Ya lo vimos en la època de los hippies y el anti americanismo pro Vietnam. Al final se salvaron aunque se perdieron por lo menos dos generaciones entre las comunas hippies y las drogas que usaron para destruir desde dentro la sociedad. Ahora están los progres con sus colectivos LGTVCX FGGHJJk, BLM y Antifa el Cristal Med y el fentanilo sin olvidarnos del antisemitismo.
Yo por los momentos sigo viendo Yellowstone, vamos a ver si esos gringos de verdad existen.
Si quieres lograr la perfección, se los mas imperfecto que puedas...
-
Axio
- Mensajes: 9176
- Registrado: Vie Ene 07, 2022 10:49 pm
- Ubicación: Ex-capitanía General de Venezuela
- Contactar:
Re: Texit: ¿Es posible la secesión de Texas?
cada pais tiene sus propias formulas para inventarse sus potes de humos.
en eeuu parece que la cosa ahora va por un muro y unos alambres de púas. que si quita el alambre porque viola derechos constitucionales del salon de la justicia, que si no lo quito porque todavía ando ardido desde la guerra civil, que si el pato y la guacharaca, etc etc etc.
luego veremos a los candidatos presidenciales hablando sobre los inmigrantes ilegales, que si el rio bravo, que si los carajitos que destetan de la mama, que si los campos de concentración para inmigrantes, es decir, todo girará en torno a la lumpen que viene llegando en masas por el patio trasero.... mientras su país se enfila derechito al despeñadero.
en eeuu parece que la cosa ahora va por un muro y unos alambres de púas. que si quita el alambre porque viola derechos constitucionales del salon de la justicia, que si no lo quito porque todavía ando ardido desde la guerra civil, que si el pato y la guacharaca, etc etc etc.
luego veremos a los candidatos presidenciales hablando sobre los inmigrantes ilegales, que si el rio bravo, que si los carajitos que destetan de la mama, que si los campos de concentración para inmigrantes, es decir, todo girará en torno a la lumpen que viene llegando en masas por el patio trasero.... mientras su país se enfila derechito al despeñadero.
La ignorancia afirma o niega rotundamente; la ciencia duda. François Marie Arouet

Re: Texit: ¿Es posible la secesión de Texas?
Y de donde sacara Texas un tercio de su presupuesto ?
Federal dollars account for one-third of the Texas state budget.
Source: Legislative Budget Board
Federal expenditures in Texas are one and a half times as much as what our state and local government revenues pay for, combined. Federal dollars account for one-third of the Texas state budget and one-tenth of preK-12 investments.
Background
Federal grants usually pay for one-third of the Texas state budget, the same as in most other states. Some, like Medicaid, foster care, or the Children’s Health Insurance Program require state or local dollars to be spent as “match” while others are a set amount based on state demographics. Federal aid is especially critical in state health and human services (almost 60 percent federally funded overall) and nutrition benefits (almost 100 percent federally funded).
Outside the state budget, Social Security and Medicare provide near-universal income support and access to health care for Texas seniors, while federal tax credits such as the Earned Income Tax Credit and Child Tax Credit are powerful anti-poverty tools.
https://everytexan.org/our-work/policy- ... get-taxes/
Federal dollars account for one-third of the Texas state budget.
Source: Legislative Budget Board
Federal expenditures in Texas are one and a half times as much as what our state and local government revenues pay for, combined. Federal dollars account for one-third of the Texas state budget and one-tenth of preK-12 investments.
Background
Federal grants usually pay for one-third of the Texas state budget, the same as in most other states. Some, like Medicaid, foster care, or the Children’s Health Insurance Program require state or local dollars to be spent as “match” while others are a set amount based on state demographics. Federal aid is especially critical in state health and human services (almost 60 percent federally funded overall) and nutrition benefits (almost 100 percent federally funded).
Outside the state budget, Social Security and Medicare provide near-universal income support and access to health care for Texas seniors, while federal tax credits such as the Earned Income Tax Credit and Child Tax Credit are powerful anti-poverty tools.
https://everytexan.org/our-work/policy- ... get-taxes/
Y lo realmente embriagador para Trump es saber lo fácil que fue convencer a la base republicana de que sus mentiras eran la verdad del evangelio.
Re: Texit: ¿Es posible la secesión de Texas?
Tu estas hablando de dinero destinado a programas sociales. Puede que Taxas fomente su propia visión de desarrollo y ya no sea necesario tanto beneficio social, con una frontera segura no se le filtre tanto pueblo buscando medicare o que los dependientes del estado se muden a San Francisco y monten una tienda de campaña y se sienten a esperar que vengan los luchadores sociales a rescatarlos y repartirles cajas clap y que lo que recibia Texas se lo manden a San Francisco para que mantenga a su lumpen..Federal grants usually pay for one-third of the Texas state budget, the same as in most other states. Some, like Medicaid, foster care, or the Children’s Health Insurance Program require state or local dollars to be spent as “match” while others are a set amount based on state demographics. Federal aid is especially critical in state health and human services (almost 60 percent federally funded overall) and nutrition benefits (almost 100 percent federally funded)
Que susto
Re: Texit: ¿Es posible la secesión de Texas?
Dentro de tu toda ignorancia sabes lo que es Medicare ?Quinoa escribió: ↑Jue Ene 25, 2024 12:00 pmTu estas hablando de dinero destinado a programas sociales. Puede que Taxas fomente su propia visión de desarrollo y ya no sea necesario tanto beneficio social, con una frontera segura no se le filtre tanto pueblo buscando medicare o que los dependientes del estado se muden a San Francisco y monten una tienda de campaña y se sienten a esperar que vengan los luchadores sociales a rescatarlos y repartirles cajas clap y que lo que recibia Texas se lo manden a San Francisco para que mantenga a su lumpen..Federal grants usually pay for one-third of the Texas state budget, the same as in most other states. Some, like Medicaid, foster care, or the Children’s Health Insurance Program require state or local dollars to be spent as “match” while others are a set amount based on state demographics. Federal aid is especially critical in state health and human services (almost 60 percent federally funded overall) and nutrition benefits (almost 100 percent federally funded)
Que susto
Y lo realmente embriagador para Trump es saber lo fácil que fue convencer a la base republicana de que sus mentiras eran la verdad del evangelio.
Re: Texit: ¿Es posible la secesión de Texas?
SI, es un programa federal destinado a personas mayores de 65 para garantizar un seguro de salud.Dentro de tu toda ignorancia sabes lo que es Medicare
Ahora si Texas se quita de encima el lobby bi partidista y se libera y consigue desarrollar su propia economía donde laboratorios inviertan y el costo de la medicina baje como en países normales y el costo de los seguros se normalice para que carrizo se van a matar por un medicare? No será mejor vivir en un.pais donde no hacen falta programas sociales y ayudas federales?
Los.socialistas como tu creen que el humano es un cerdo al que hay que tirarle los restos y solo pueden sobrevivir de a caridad del amo.
Crean el problema y luegon os hacen dependientes de migajas
-
Senderos
- Mensajes: 8853
- Registrado: Dom Dic 12, 2021 3:59 pm
- Ubicación: https://www.mossad.gov.il/
- Contactar:
Re: Texit: ¿Es posible la secesión de Texas?
Texas independiente nonecesitaría de presupuesto federal, podría aplicar sus propias politicas de como utilizar sus ingresos y a quien, recortando gastos donde no se necesita para redistribuirlos a los texanos de verdad... solo un tercio apenas? eso no es nada.Lander escribió: ↑Jue Ene 25, 2024 11:34 am Y de donde sacara Texas un tercio de su presupuesto ?
Federal dollars account for one-third of the Texas state budget.
Source: Legislative Budget Board
Federal expenditures in Texas are one and a half times as much as what our state and local government revenues pay for, combined. Federal dollars account for one-third of the Texas state budget and one-tenth of preK-12 investments.
Background
Federal grants usually pay for one-third of the Texas state budget, the same as in most other states. Some, like Medicaid, foster care, or the Children’s Health Insurance Program require state or local dollars to be spent as “match” while others are a set amount based on state demographics. Federal aid is especially critical in state health and human services (almost 60 percent federally funded overall) and nutrition benefits (almost 100 percent federally funded).
Outside the state budget, Social Security and Medicare provide near-universal income support and access to health care for Texas seniors, while federal tax credits such as the Earned Income Tax Credit and Child Tax Credit are powerful anti-poverty tools.
https://everytexan.org/our-work/policy- ... get-taxes/
Jews Are The Only Indigenous of The Ancestral Land of Israel
Re: Texit: ¿Es posible la secesión de Texas?
Lander.me.recuerda a los chavistas amenazando al pueblo de que si votan por la oposicion les quitan las cajas clap y los bonos.ita para redistribuirlos a los texanos de verdad
A mi eso me da asco, como es posible que conviertan a la gente en mendigos para luego autonombrarse los salvadores?
-
Senderos
- Mensajes: 8853
- Registrado: Dom Dic 12, 2021 3:59 pm
- Ubicación: https://www.mossad.gov.il/
- Contactar:
Re: Texit: ¿Es posible la secesión de Texas?
Los regres Están ayudando a destruir a Estados Unidos desde dentro y parecen estar orgullosos y mucho más ma.ldito que un progre es un progre venezolano, si USA no modifica el rumbo la independencia se vuelve una necesidad vital para Texas otros estados.Quinoa escribió: ↑Jue Ene 25, 2024 1:28 pmLander.me.recuerda a los chavistas amenazando al pueblo de que si votan por la oposicion les quitan las cajas clap y los bonos.ita para redistribuirlos a los texanos de verdad
A mi eso me da asco, como es posible que conviertan a la gente en mendigos para luego autonombrarse los salvadores?
Se independizan o se mueren convirtiendose en shitholes socialistas tercermundistas.
Jews Are The Only Indigenous of The Ancestral Land of Israel
-
verdinegro
- Mensajes: 15294
- Registrado: Sab Dic 18, 2021 10:30 am
- Ubicación: Evropa
- Contactar:
Re: Texit: ¿Es posible la secesión de Texas?
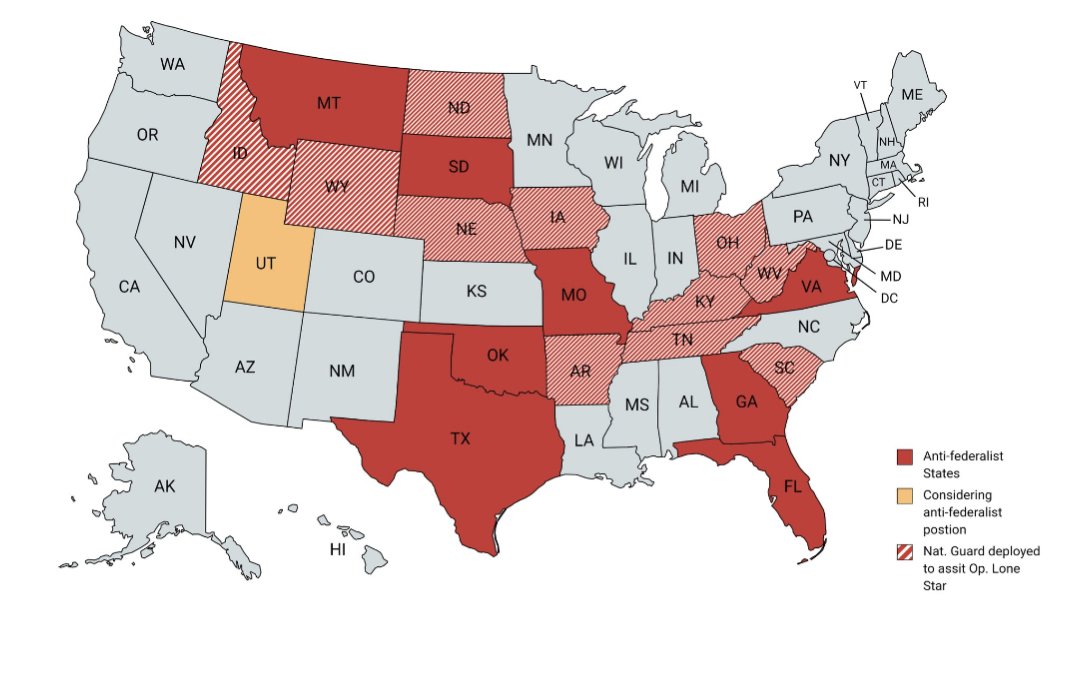
Una marea roja rojita. 
Re: Texit: ¿Es posible la secesión de Texas?
Hablar de estos temas sin revisar la importancia de lo que esta pasando...es hablar por hablar.
Taxas y Florida aportan practicamente el 20% del PIB de USA y entre los 15 estados alebrestados mas de el 68%...cualquier cosita u la economia se va a la mielda...
No digo mas...
Taxas y Florida aportan practicamente el 20% del PIB de USA y entre los 15 estados alebrestados mas de el 68%...cualquier cosita u la economia se va a la mielda...
No digo mas...
Si quieres lograr la perfección, se los mas imperfecto que puedas...
Re: Texit: ¿Es posible la secesión de Texas?
Más nada que decir....medicare? NMJTaxas y Florida aportan practicamente el 20% del PIB de USA y entre los 15 estados alebrestados mas de el 68%...cualquier cosita u la economia se va a la mielda

Re: Texit: ¿Es posible la secesión de Texas?
Mas interesados en secesión,
son los siberianos.
Que viven en ranchos,
de la epoca del zar,
cuando son el territorio mas rico de Rusia.
He construído castillos tan hermosos en mis sueños, que sólo con las ruinas me conformaría.
Re: Texit: ¿Es posible la secesión de Texas?
Supongo que Israel es un pais socialista y que dan cajas clap y bonos por ofrecer a TODOS sus cuidadanos un sistema de salud universal.
Cual es el problema de dar salud a los mayores de 65 años cuando es evidentemente mas costoso que vayan a salas de emergencia, o prefieren que se mueran por no poder pagar una consulta o una medicina?
Que clase de gente son algunos de los que escriben por aca?
Increible.
List of countries with universal health care
From Wikipedia, the free encyclopedia
Government-guaranteed health care for all citizens of a country, sometimes called universal health care, is a broad concept that has been implemented in several ways. The common denominator for all such programs is some form of government action aimed at broadly extending access to health care and setting minimum standards. Most implement universal health care through legislation, regulation, and taxation. Legislation and regulation direct what care must be provided, to whom, and on what basis.
The logistics of such health care systems vary by country. Some programs are paid for entirely out of tax revenues. In others, tax revenues are used either to fund insurance for the very poor or for those needing long-term chronic care. In some cases such as the UK, government involvement also includes directly managing the health care system, but many countries use mixed public-private systems to deliver universal health care. Alternatively, much of the provision of care can be contracted from the private sector, as in the case of Canada and France. In some instances, such as in Italy and Spain, both these realities may exist at the same time. The government may provide universal health insurance in the form of a social insurance plan that is affordable by all citizens, such as in the case of Germany and Taiwan, although private insurance may provide supplemental coverage to the public health plan. In twenty-five European countries, universal healthcare entails a government-regulated network of private insurance companies.[1][2]
As of 2021, Brazil is the only country where any individual within the state's jurisdiction is eligible to receive free healthcare with no previous application, which covers all treatments, surgeries, and medications at any condition, whether resident or non-resident, regardless of ethnicity, nationality, or visa, including tourists, passengers in transit, and refugees.[3]
Africa
Algeria
Algeria operates a public healthcare system. It is a universal healthcare system as well. A network of hospitals, clinics, and dispensaries provide treatment to the population, with the Social Security system funding health services, although many people must still cover part of their costs due to the rates paid by the Social Security system remaining unchanged since 1987. The poor are generally entitled to taxpayer funded health services, while the wealthy pay for treatment according to a sliding scale.[4][5]
Botswana
Main article: Health in Botswana
Botswana established a free healthcare system that operates a system of public medical centers, with 98% of health facilities in the country run by the government.[citation needed] All citizens are entitled to be treated in taxpayer funded facilities, though a nominal fee of ~70 BWP (~US$6.60) is typically charged for public health services except for sexual reproductive health services and antiretroviral therapy services, which are free.[6]
Burkina Faso
Burkina Faso provides universal healthcare to citizens through a system called Universal Health Insurance (AMU)—administered by two bodies, one for civilians and the other for the armed forces.[7]
Mauritius
The Government of Mauritius operates a system of medical facilities that provide treatment to citizens free of charge.[8]
Morocco
Morocco does not have universal health care. It is currently building a system which was slated to cover the entire population by the end of 2022.[9] The country operates a public health sector run by the government that operates 85% of the country's hospital beds. It deals mainly with the poor and rural populations, who cannot afford private healthcare. In addition, a non-profit health sector operated by the National Social Security Fund covers 16% of the population. Private medical care is available for those who can afford it.[10]
Rwanda
Main article: Healthcare in Rwanda
Rwanda operates a system of universal health insurance through the Ministry of Health called Mutuelle de Santé (Mutual Health), a system of community-based insurance where people pay premiums based on their income level into local health insurance funds, with the wealthiest paying the highest premiums and required to cover a small percentage of their medical expenses, while those at the lowest income levels are exempt from paying premiums and can still utilize the services of their local health fund. In 2012, this system insured all but 4% of the population.[11]
Seychelles
The government of Seychelles operates a system of medical facilities that provide treatment to citizens free of charge.
Tunisia
Tunisia operates a public healthcare system under the National Health Insurance Fund (Caisse Nationale d'Assurance Maladie). All Tunisian citizens and residents can receive treatment in state-run hospitals and clinics for a very low co-pay, while people with the lowest income are able to apply for an exemption from co-pays.[12]
Asia
Countries and regions that provide public healthcare in Asia include Bangladesh, Bhutan,[13] Bahrain,[14] Brunei, China, Hong Kong, India, Indonesia,[15] Iran,[16] Israel[17] (see below), Jordan,[18] Kazakhstan,[19] Macau (see below), Malaysia,[20] Mongolia,[21] Oman,[22] Pakistan (KPK),[23] Philippines,[24] Singapore, Qatar, DPRK (North Korea),[25] Sri Lanka,[26] Syria,[27] Taiwan (R.O.C.)[28] (see below), Japan, South Korea, and Saudi Arabia.
Bhutan
Main article: Health in Bhutan
The Royal Government of Bhutan maintains a policy of free and universal access to primary health care. As hospital facilities in the country are limited, patients with diseases that cannot be treated in Bhutan, such as cancer, are normally referred to hospitals in India for treatment. Such referral treatment is also carried out at the cost of the Royal Government.[29]
China
Main article: Healthcare reform in China
As of 2017, more than 97% of people in China are covered by one of three categories of public health insurance. From most generous to least generous, they are the:
Urban Employee Basic Medical Insurance (UEBMI, 职工医保)
Urban Resident Basic Medical Insurance (URBMI, 居民医保)
New Cooperative Medical Service (NCMS, 新农合)
The UEBMI is funded by 6-12% by employers and 2% by employees; the URBMI entirely by local governments, and it covers students, the unemployed, and the retired; and the NCMS by the central government. In 2016, the government announced plans to merge NCMS with URBMI. China also has five private health insurance companies for supplementary care: the three largest are Ping An, PICC, and China Life. [30] For the public plans, the list of covered procedures is limited, and copayment is common. The proportion of out-of-pocket costs depends on profession and location: for example, workers in urban Shanghai might have 85% of their medical costs covered up to $740,000 while workers in rural Guiyang are reimbursed for 65% of their medical costs up to $29,000 annually.[31]
Immediately after the Chinese Communist Revolution in 1949, the state both directly operated all hospitals and clinics. The government paid for healthcare services, and life expectancy improved greatly, although the services provided were basic. State-provided health insurance varied by area: the Cooperative Medical System (CMS) covered rural areas, while the Government Insurance Scheme (GIS) and Labor Insurance Scheme (LIS) covered residents of urban areas.[32] After the Chinese economic reform in 1978, the state reduced spending on hospitals and allowed them to charge patients for profit. The state, however, did not stop paying for certain healthcare services like mandatory vaccination.[31]
From the high point of privatization of healthcare in the 1990s,[32] China has been reforming with universal health care as a goal in the 21st century, as part of the "moderately prosperous society" plan. The New Rural Co-operative Medical Care System (NRCMCS) from 2005, aimed at the rural poor, sets the annual cost of medical coverage at 50 yuan (US$7) per person. As of September 2007, around 80% of the whole rural population of China had signed up (about 685 million people). For patients who go to a small hospital or clinic in their local town, the scheme covers from 70 to 80% of their bill; patients at a county provider get 60% of their cost covered; and in a large modern city hospital, the scheme covers about 30% of the bill.[33]
At the end of 2008, the government published its reform plan clarifying government's responsibility by saying that it would play a dominant role in providing public health and basic medical service. The plan listed public health, rural areas, city community health services and basic medical insurance as four key areas for government investment. It also promised to tighten government control over medical fees in public hospitals and to set up a "basic medicine system" to cover drug costs.[34][35] China's "Law on Promotion of Basic Medical and Health Care", effective June 2020, asserts that Chinese citizens have a positive right to healthcare, regardless of cost. Additional laws are expected to specify what this right will mean in practice.[citation needed]
Hong Kong
Main article: Health in Hong Kong
Hong Kong has early health education, professional health services, and well-developed health care and medication system. The life expectancy is 84 for females and 78 for males,[36] which is the second highest in the world, and 2.94 infant mortality rate, the fourth lowest in the world.[37][38]
There are two medical schools in Hong Kong, and several schools offering courses in traditional Chinese medicine. The Hospital Authority is a statutory body that operates and manages all public hospitals. Hong Kong has high standards of medical practice. It has contributed to the development of liver transplantation, being the first in the world to carry out an adult to adult live donor liver transplant in 1993.[39]
India
Main article: Healthcare in India
At the federal level, a national health insurance program was launched in 2018 by the Government of India, called Ayushman Bharat. This aimed to cover the bottom 50% (500 million people) of the country's population working in the unorganized sector (enterprises having less than 10 employees) and offers them free treatment at both public and private hospitals.[40] For people working in the organized sector (enterprises with more than 10 employees) and earning a monthly salary of up to Rs 21000 are covered by the social insurance scheme of Employees' State Insurance which entirely funds their healthcare (along with pension and unemployment benefits), both in public and private hospitals.[41][42] People earning more than that amount are provided health insurance coverage by their employers through the many public or private insurance companies. As of 2020, 300 million Indians are covered by insurance bought from one of the public or private insurance companies by their employers as group or individual plans.[43] Unemployed people without coverage are covered by the various state insurance schemes if they do not have the means to pay for it.[44] In 2019, the total net government spending on healthcare was $36 billion or 1.23% of its GDP.[45] An outpatient card at AIIMS costs a one-time fee of 10 rupees (around 20 cents U.S.) and thereafter outpatient medical advice is free. In-hospital treatment costs is extremely minimal and depends on the financial condition of the patient and the facilities utilized, but are usually much less than in the private sector. For instance, a patient is waived treatment costs if their income is below the poverty line. However, getting treatment at high quality government hospitals is very tough due to the high number of people needing healthcare and the lack of sufficient facilities.
Primary health care is provided by city and district hospitals and rural primary health centres (PHCs). These hospitals provide treatment free of cost. Primary care is focused on immunization, prevention of malnutrition, pregnancy, child birth, postnatal care, and treatment of common illnesses.[46] Patients who receive specialized care or have complicated illnesses are referred to secondary (often located in district and taluk headquarters) and tertiary care hospitals (located in district and state headquarters or those that are teaching hospitals).[citation needed]. In urban cities and towns like Delhi, there are neighbourhood health clinics called Mohalla Clinics which offer completely free treatment, testing and drugs.[47]
The Indian government has launched Ayushyaman Bharat Yojana (AB-NHPM), which will provide all Indian citizens with insurance coverage for serious illnesses, and free drugs and diagnostic treatments.[48]
Indonesia
Main article: Healthcare in Indonesia
Indonesia is currently building a universal healthcare system with its Jaminan Kesehatan Nasional (JKN) scheme, managed by BPJS Kesehatan, which covers a range of treatments from public providers as well as private providers that opt to participate. The scheme is funded by premiums from the employed. The formally employed pay a premium worth 5% of their salary, with 1% paid by the employee and 4% paid by the employer, while informal workers and the self-employed must pay a fixed monthly premium. As of April 2018, 75% of the population was covered by JKN.[49]
While the country has a number of government-owned hospitals, about 63% are privately owned.[50] Indonesia also operates a three-tier community health system. The Ministry of Health oversees a network of Puskesmas, or community health centers, followed by health sub-centers and village-level integrated posts.[51]
Israel
Main article: Healthcare in Israel
Health care in Israel as a percentage of GDP
Israel has a system of universal healthcare as set out by the 1995 National Health Insurance Law. The state is responsible for providing health services to all residents of the country, who can register with one of the four national health service funds. To be eligible, a citizen must pay a health insurance tax. Coverage includes medical diagnosis and treatment, preventive medicine, hospitalization (general, maternity, psychiatric and chronic), surgery and transplants, preventive dental care for children, first aid and transportation to a hospital or clinic, medical services at the workplace, treatment for drug abuse and alcoholism, medical equipment and appliances, obstetrics and fertility treatment, medication, treatment of chronic diseases and paramedical services such as physiotherapy and occupational therapy.[52]
In Israel, the National Health Insurance Law is the legal framework that enables and facilitates basic, compulsory universal health care. Promoted by health minister Haim Ramon in the early 1990s,[53] the Knesset put the law into effect on January 1, 1995—basing it on recommendations from a National Committee of Inquiry headed by Shoshana Netanyahu, which examined restructuring the health care system in Israel in the late 1980s. Prior to the law's passage, over 90% of the population was already covered by voluntarily belonging to one of four nationwide, not-for-profit sickness funds. These operated some of their own medical facilities, funded in part by employers and the government, and in part by the insured via levies that varied according to income. However, there were three problems associated with this arrangement. First, membership in the largest fund, Clalit, required one to belong to the Histadrut labor organization, even if a person did not want to (or could not) have such an affiliation, and other funds restricted entry to new members based on age, pre-existing conditions, or other factors. Second, different funds provided different levels of benefit coverage or services to their members. Lastly, some of the population, albeit a small percentage, had no health insurance.
Before the law went into effect, all the funds collected premiums directly from members. However, upon passage of the law, a new progressive national health insurance tax was levied through Bituah Leumi (Israel's social security agency), which then re-distributes the proceeds to the sickness funds based on their membership and its demographic makeup. This ensured that all citizens would now have health coverage. While membership in one of the funds now became compulsory for all, free choice was introduced into movement of members between funds (a change is allowed once every six months), effectively making the various sickness funds compete equally for members among the populace. Annually, a committee appointed by the ministry of health publishes a "basket" or uniform package of medical services and prescription formulary that all funds must provide as a minimum to all members. Achieving this level of equality guaranteed basic healthcare regardless of fund affiliation, which was one of the principal aims of the law. An appeals process handles rejection of treatments and procedures by the funds and evaluates cases that fall outside the "basket" of services or prescription formulary.
The law is generally considered a success, and Israeli citizens enjoy a high standard of medical care comparatively, with more competition in the country's health care, and with order having brought to what was once a somewhat disorganized system—the law nevertheless has its critics. First among the criticisms is that the "basket" may not provide enough coverage. To partly address this, the health funds began offering "supplementary" insurance to cover certain additional services not in the basket. However, since this insurance is optional (though rather modestly priced, costing the equivalent of about US$10 to $35 a month depending on age and coverage for an adult in 2019), critics argue that it goes against the spirit of the new law, which stressed equality of healthcare for all citizens. Another criticism is that, to provide universal coverage to all, the tax income base amount (the maximum amount of yearly earnings that are subject to the tax) was set rather high, causing many high-income taxpayers to see the amount they pay for their health premiums (now health tax) skyrocket. Finally, some complain about the constantly rising costs of copayments for certain services.
Japan
Main article: Health care system in Japan
All residents of Japan are required by the law to have health insurance coverage. People without insurance from employers can participate in a national health insurance programme, administered by local governments. Patients are free to select physicians or facilities of their choice and cannot be denied coverage. Hospitals, by law, must be run as non-profit and be managed by physicians.
Kuwait
Main article: Healthcare in Kuwait
Kuwait offers universal healthcare.
Macau
Main article: Healthcare in Macau
Macau offers universally accessible single-payer system funded by taxes. Health care is provided by the Health Bureau.
Malaysia
Malaysia has achieved universal health coverage. It has made remarkable progress in improving health outcomes over the past seven decades. At the time of Independence, the number of infant deaths was 75.5 per 1,000 live births. This has since fallen by more than 90 percent to 6.7 deaths per 1,000 live births in 2016. Maternal mortality which refers to the death of a woman caused by her pregnancy, during and after delivery, has also decreased by 89% between 1963 and 2013.[54]
Maldives
Aasandha is the national healthcare insurance scheme of the Maldives. It provides taxpayer-funded medical assistance to all Maldivian citizens. National Social Protection Agency of Maldives was formed under the National Social Health Insurance Act on August 27, 2008. It is mandated to administer the National Social Health Insurance Scheme and by an executive order under the same act mandated to conduct social protection programs identified by the government of Maldives. NSPA is also the responsible agency to regulate and conduct Social Protection programs under the Social Protection Act.
Pakistan
In Pakistan, Universal Healthcare exists on provincial levels, started by the Government of Khyber Pakhtunkhwa, which had launched a "universal health insurance programme" known as the "Sehat Insaf Card" to provide free healthcare for the residence of KPK, where families would be covered up to Rs. 10 lakh (US$3,500) for treatment.[23] This was further expanded to the Punjab province of Pakistan, in December 2021, to cover more than 31 million families. Prime Minister Imran Khan announced that an additional Rs. 440 billion (US$1.5 billion) would be spent to cover the entire province.[55]
Philippines
Filipinos are covered under the National Health Insurance Program (NHIP) of the Philippine government-owned Philippine Health Insurance Corporation or PhilHealth. Under the Universal Health Care Law of 2019, all Filipinos were automatically enrolled in the NHIP.[56]
Saudi Arabia
The Government of Saudi Arabia provides free universal health coverage for all citizens. Non-citizens are required by law to have private insurance paid for by their employer.
Singapore
Main article: Healthcare in Singapore
Singapore has a universal health care system where government ensures affordability, largely through compulsory savings and price controls, while the private sector provides most care. Overall spending on health care amounts to only 3% of annual GDP. Of that, 66% comes from private sources.[57] Singapore currently has the second lowest infant mortality rate in the world and among the highest life expectancies from birth, according to the World Health Organization.[58] Singapore has "one of the most successful healthcare systems in the world, in terms of both efficiency in financing and the results achieved in community health outcomes," according to an analysis by global consulting firm Watson Wyatt.[59] Singapore's system uses a combination of compulsory savings from payroll deductions (funded by both employers and workers) a nationalized health insurance plan, and government subsidies, as well as "actively regulating the supply and prices of healthcare services in the country" to keep costs in check; the specific features have been described as potentially a "very difficult system to replicate in many other countries." Many Singaporeans also have supplemental private health insurance (often provided by employers) for services not covered by the government's programs.[59]
South Korea
Main article: Healthcare in South Korea
South Koreans have access to a universal healthcare safety net, although a significant portion of healthcare is privately funded.
North Korea
Main article: Health in North Korea
North Korea claims to provide universal health care with a national medical service and health insurance system.[60] It claims that health services are offered for free.[60]: 7–8 However, this claim has been contrasted by North Korean defectors, who claim that patients must in fact pay for health services, that the upper classes have access to a higher standard of healthcare than ordinary ones do, and that "how much money a patient has determines whether they live or die".[61]
Sri Lanka
Main article: Healthcare in Sri Lanka
Sri Lanka provides free universal healthcare to their citizens.[62]
Taiwan
Main article: Healthcare in Taiwan
The current health care system in Taiwan, known as National Health Insurance (NHI), was instituted in 1995. NHI is a single-payer compulsory social insurance plan that centralizes the disbursement of health care dollars. The system promises equal access to health care for all citizens, and the population coverage had reached 99% by the end of 2004.[63] NHI is mainly financed through premiums based on the payroll tax, and is supplemented with out-of-pocket payments and direct government funding. In the initial stage, fee-for-service predominated for both public and private providers.[citation needed]
NHI delivers universal coverage offered by a government-run insurer. The working population pays premiums split with their employers, others pay a flat rate with government help and the poor or veterans are fully subsidized.[64]
Under this model, citizens have free range to choose hospitals and physicians without using a gatekeeper and do not have to worry about waiting lists. NHI offers a comprehensive benefit package that covers preventive medical services, prescription drugs, dental services, Chinese medicine, home nurse visits and many more. Since NHI, the previously uninsured have increased their usage of medical services. Most preventive services are free such as annual checkups and maternal and child care. Regular office visits have co-payments as low as US$5 per visit. Co-payments are fixed and unvaried by the person's income.[65]
Thailand
Main article: Healthcare in Thailand
Thailand introduced universal coverage reforms in 2001, becoming one of only a handful of lower-middle income countries to do so at the time. Means-tested health care for low income households was replaced by a new and more comprehensive insurance scheme, originally known as the 30 baht project, in line with the small co-payment charged for treatment. People joining the scheme receive a gold card that they use to access services in their health district, and, if necessary, get referrals for specialist treatment elsewhere. The bulk of finance comes from public revenues, with funding allocated to Contracting Units for Primary Care annually on a population basis. According to the WHO, 65% of Thailand's health care expenditure in 2004 came from the government, and 35% was from private sources.[57] Although the reforms have received a good deal of critical comment, they have proved popular with poorer Thais, especially in rural areas, and survived the change of government after the 2006 military coup. The then Public Health Minister, Mongkol Na Songkhla, abolished the 30 baht co-payment and made the UC scheme free. It is not yet clear whether the scheme will be modified further under the coalition government that came to power in January 2008.[66][67][68]
In 2016, Thailand became the first country in Asia to eliminate HIV transmission from mother to child, owing to its robust public healthcare system.[69]
United Arab Emirates
Main article: Healthcare in the United Arab Emirates
The United Arab Emirates has enacted federal legislation that requires universal healthcare nationals and mandatory health insurance for expatriates, but this legislation has not yet been implemented across the entire country. [70]
Europe
Main article: Healthcare in Europe
Almost all European countries have healthcare available for all citizens. Most European countries have systems of competing private health insurance companies, along with government regulation and subsidies for citizens who cannot afford health insurance premiums.[71] Countries with universal healthcare include Austria, Belarus,[72] Bulgaria, Croatia, Czech Republic, Denmark, Finland, France, Germany, Greece, Iceland, Italy, Latvia, Lithuania, Luxembourg, Macedonia, Malta, Moldova,[73] Norway, Poland, Portugal,[74] Romania, Russia, Serbia, Spain, Sweden, Switzerland, Ukraine,[75] and the United Kingdom.[76]
Albania
Main article: Healthcare in Albania
Healthcare in Albania is universal for citizens of Albania.
Armenia
Main article: Healthcare in Armenia
Armenia operates a mandatory social health insurance system. The majority of the population is enrolled in the Compulsory Health Insurance Fund, which is funded through payroll taxes and contributions from employers and employees.
Austria
Main article: Healthcare in Austria
Healthcare in Austria is universal for residents of Austria as well as those from other EU countries.[77] Austria has a two-tier payment system in which many individuals receive basic publicly funded care; they also have the option to purchase supplementary private health insurance.
Belgium
Main article: Healthcare in Belgium
Healthcare in Belgium is composed of three parts. Firstly there is a primarily publicly funded healthcare and social security service run by the federal government, which organises and regulates healthcare; independent private/public practitioners, university/semi-private hospitals and care institutions. There are a few (commercially run for-profit) private hospitals.[78] Secondly is the insurance coverage provided for patients. Finally, industry coverage covers the production and distribution of healthcare products for research and development. The primary aspect of this research is done in universities and hospitals.
Bulgaria
Healthcare in Bulgaria is mixed. Some services are private, like dental care, and some services are run publicly by NHIF.[79] Because 15% of the population is uninsured and cannot access most health services, it does not currently qualify as having universal healthcare.[80]
Croatia
Main article: Healthcare in Croatia
Croatia has a universal health care system that provides medical services and is coordinated by the Ministry of Health. The population is covered by a basic health insurance plan provided by statute and by optional insurance. It is administered by the Croatian Health Insurance Fund. In 2012, annual compulsory healthcare related expenditures reached 21.0 billion kunas (c. 2.8 billion euro). There are hundreds of healthcare institutions in Croatia, including 79 hospitals and clinics with 25,285 beds, caring for more than 760 thousand patients per year, 5,792 private practice offices and 79 emergency medical service units.
Cyprus
Main article: Health care in Cyprus
A universal national health system, known as GESY, was implemented in Cyprus in June 2019. The new system aims to provide affordable and effective medical care to all people residing permanently in Cyprus. As of June 2022, 917,000 Cypriots have registered[5][clarification needed] with a general practitioner through the GESY system, which is roughly the current population of the Republic of Cyprus.
Czech Republic
Main article: Healthcare in the Czech Republic
Czech Republic has a universal public health system paid largely from taxation. Private health care systems do co-exist freely alongside public ones, sometimes offering better quality or faster service. Almost all medical services are covered by health insurance and insurance companies, though certain services such as prescription drugs or vision and dental care are only covered partially.
Denmark
Main article: Health care in Denmark
Denmark has a universal public health system paid largely from taxation with local municipalities delivering health care services in the same way as other Scandinavian countries. Primary care is provided by a general practitioner service run by private doctors contracting with the local regions with payment on a mixed per capita and fee for service basis. Most hospitals are run by the regions (only 1% of hospital beds are in the private sector).
Estonia
Main article: Healthcare in Estonia
Estonia's health care system is based on compulsory insurance based on solidarity funding and on universal access to services provided by private service providers.
Finland
Main article: Healthcare in Finland
In Finland, public medical services at clinics and hospitals are run by the municipalities (local government) and are funded 76% by taxation, 20% by patients through access charges, and 4% by others. Private provision is mainly in the primary care sector. There are a few private hospitals.[81] The main hospitals are either municipally owned (funded from local taxes) or run by the medical teaching universities (funded jointly by the municipalities and the national government). According to a survey published by the European Commission in 2000, Finland's is in the top 4 of EU countries in terms of satisfaction with their hospital care system: 88% of Finnish respondents were satisfied compared with the EU average of 41.3%.[82] Finnish health care expenditures are below the European average.[83] The private medical sector accounts for about 14 percent of total health care spending. Only 8% of doctors choose to work in private practice, and some of these also choose to do some work in the public sector.[citation needed]
Taxation funding is partly local and partly nationally based. The national social insurance institution KELA reimburses part of patients prescription costs and makes a contribution towards private medical costs (including dentistry) if they choose to be treated in the private sector rather than the public sector. Patient access charges are subject to annual caps. For example, GP visits cost €11 per visit with annual €33 cap; hospital outpatient treatment €22 per visit; a hospital stay, including food, medical care and medicines €26 per 24 hours, or €12 if in a psychiatric hospital. After a patient has spent €683 per year on public medical services, all further treatment in that year is covered (although the required initial deductible is reviewed annually, so it may vary). There is a separate reimbursement system for prescribed medicine: after paying €578 per year, the remaining bought medicine will have a maximum price of €2.50 per purchase.[84]
Finland has a highly decentralized three-level public system of health care and alongside this, a much smaller private health care system.[85] Overall, the municipalities (funded by taxation, local and national) meet about two thirds of all medical care costs, with the remaining one third paid by the national insurance system (nationally funded), and by private finance (either employer-funded or met by patients themselves).[85] Private inpatient care forms about 3–4% of all inpatient care.[85] In 1999 only 17 per cent of total funding for health care came from insurance, comprising 14.9% statutory (government) insurance and 2.1% private health insurance. Eyeglasses are not publicly subsidized at all, although dentistry is available as a municipal service or can be obtained privately with partial reimbursement from the state.[85]
The percentage of total health expenditure financed by taxation in Finland (78%)[86] is above the OECD average and similar to the levels seen in Germany (77%) and France (80%) but below the level seen in the UK (87%). The quality of service in Finnish health care, as measured by patient satisfaction, is excellent. According to a survey published by the European Commission in 2000, Finland has one of the highest ratings of patient satisfaction with their hospital care system in the EU: 88% of Finnish respondents were satisfied compared with the EU average of 41.3%.[87]
There are caps on total medical expenses that are met out-of-pocket for drugs and hospital treatments. The National Insurance system pays all necessary costs over these caps. Public spending on health care in 2006 was 13.6 billion euros (equivalent to US$338 per person per month). The increase over 2005 at 8.2 per cent was below the OECD average of 9 percent. Household budgets directly met 18.7 per cent of all health care costs.[88]
France
Main article: Health care in France
France has a system of health care largely financed by government through a system of national health insurance. Nonetheless, not all medical care is paid for by the state, with only 70% of initial GP care covered and anywhere between 35% and 100% of prescription medication covered. It is consistently ranked as one of the best in the world.[89]
Georgia
Main article: Healthcare in Georgia (country)
In 2013, Georgia adopted a universal health care system. Healthcare in Georgia is provided by a universal health care system under which the state funds medical treatment in a mainly privatized system of medical facilities. In 2013, the enactment of a universal health care program triggered universal coverage of government-sponsored medical care of the population and improving access to health care services. Responsibility for purchasing publicly financed health services lies with the Social Service Agency (SSA).[90][91] However, according to the UN, due to the high out-of-pocket costs that patients incur, Georgia has not yet achieved universal healthcare.[92]
Germany
Main article: Health care in Germany
The Charité (Hospital) in Berlin
Germany has the world's oldest national social health insurance system,[93][94][95] with origins dating back to Otto von Bismarck's Sickness Insurance Law of 1883.[96][97] The system is decentralized with private practice physicians providing ambulatory care, and independent, mostly non-profit hospitals providing the majority of inpatient care. Employers pay for half of their employees' health insurance contributions, while self-employed workers pay the entire contribution themselves.[98] Approximately 90% of the population is covered by a statutory health insurance plan, which provides a standardized level of coverage through any one of approximately 100 public sickness funds.[98][99] The rest are covered by private health insurance. Private health insurance is only accessible to self-employed workers, high-income employees and Beamte. The contributions for public insurance is determined according to income, while the contributions for private health insurance are determined according to age and health condition.[98]
Purchasing basic health insurance is mandatory for all persons residing in Germany if not employed. Historically, the level of provider reimbursement for specific services is determined through negotiations between regional physician's associations and sickness funds. Since 1976 the government has convened an annual commission, composed of representatives of business, labor, physicians, hospitals, and insurance and pharmaceutical industries.[100] The commission takes into account government policies and makes recommendations to regional associations with respect to overall expenditure targets. In 1986 expenditure caps were implemented and were tied to the age of the local population as well as the overall wage increases. Although reimbursement of providers is on a fee-for-service basis, the amount to be reimbursed for each service is determined retrospectively to ensure that spending targets are not exceeded. Capitated care, such as that provided by U.S. health maintenance organizations, has been considered as a cost containment mechanism but would require consent of regional medical associations, and has not materialized.[101]
Copayments were introduced in the 1980s in an attempt to prevent overutilization and control costs. The average length of hospital stay in Germany has decreased in recent years from 14 days to 9 days, still considerably longer than average stays in the U.S. (5 to 6 days).[102][103] The difference is partly driven by the fact that hospital reimbursement is chiefly a function of the number of hospital days as opposed to procedures or the patient's diagnosis. Drug costs have increased substantially, rising nearly 60% from 1991 through 2005. Despite attempts to contain costs, overall health care expenditures rose to 10.7% of GDP in 2005, comparable to other western European nations, but substantially less than that spent in the U.S. (nearly 16% of GDP).[104]
Greece
Main article: Healthcare in Greece
The Greek healthcare system provides high quality medical services to insured citizens and is coordinated by the Ministry for Health and Social Solidarity. Public health services are provided by the National Healthcare Service, or ESY (Greek: Εθνικό Σύστημα Υγείας, ΕΣΥ). In 2010 there were 35,000 hospital beds and 131 hospitals in the country.
The Greek healthcare system has received high rankings by the World Health Organization, ranked 14th in the overall assessment and 11th in quality of service in a 2000 report by the WHO. However, it must be noted that the entire financial system collapsed in 2007–2008. The data listed above is from 2000.
Iceland
Main article: Healthcare in Iceland
Iceland has a universal public health system paid largely from taxation with local municipalities delivering health care services in the same way as the Scandinavian countries. Iceland's entire population has equal access to health care services.[citation needed][105]
Ireland
Main article: Healthcare in the Republic of Ireland
The public health care system in Ireland is governed by the Health Act 2004,[106] which established a new body to be responsible for providing health and personal social services to everyone living in Ireland – the Health Service Executive. The new national health service came into being officially on January 1, 2005; however, the new structures are currently[when?] in the process of being established as the reform program continues[citation needed]. In addition to the public-sector, there is a large private health care market.
In Ireland, 37% of the population have a means-tested medical card that gives the holder access to tax-funded GP care and requires €2.00 for each prescription drug.[107] The standard charge for Irish and EU citizens who attend the A&E in hospitals is €100. This is free of charge if referred by a GP.[108] For all other residents who do not have a medical card, the average price for an appointment with a family doctor GP is €50 or €70 for an emergency appointment with a Caredoc GP.[109] Ireland is currently in the process of establishing a universal healthcare system based on compulsory private health insurance, with competition managed by the government. These reforms are known as Sláintecare and are scheduled to be completed by 2030.[110]
Italy
Main article: Healthcare in Italy
Italy has a public health care service for all the residents called "Servizio Sanitario Nazionale" or SSN (National Health Service). It is publicly run and funded mostly by taxation. Some services require variable co-pays, while other services (such as emergency medicine and a general doctor) are free. There is also a small parallel private health care system, especially in the field of dentistry and optometry.
Latvia
Main article: Healthcare in Latvia
Healthcare in Latvia is universal for citizens of Latvia. The healthcare system in Latvia operates as a universal program that is primarily funded through government taxation.[111] It bears similarities to the National Health Service (NHS) in UK and employs a purchaser-provider split (PPS). Following several reforms, a National Health Service (NHS) type system, known as Nacionālais veselības dienests (NVD) in Latvian, was established in 2011.[112]
The NVD controls the implementation of healthcare policies while the Ministry of Health develops policies and oversees the system. Healthcare services are available for free for citizens of Latvia. The country's Ministry of Health manages its healthcare system through a combination of social insurance institutional body, legislative healthcare provision financed by taxes and numerous public and private providers.[113]
Despite near-universal population coverage provided by the NVD established in 2011, there are challenges to equitable access with issues around geographical distribution of health professionals, user charges and long waiting lists. The publicly funded health benefits package is limited in scope and only covers a predetermined set of services.[114][115]
Lithuania
Main article: Healthcare in Lithuania
The public healthcare system in Lithuania ensures free healthcare for almost all its citizens. This state-funded healthcare is available to long-term residents and expats too.
Luxembourg
Main article: Healthcare in Luxembourg
Luxembourg provides universal health care coverage to all residents (Luxembourgers and foreigners) by the National Health Insurance (CNS - Caisse nationale de santé (French) or National Gesondheetskeess (Luxembourgish)). It is funded by mandatory contributions of employers and the workforce, and by government subsidies for insuring jobseekers, the poor, and for financing medical infrastructure. The nation also has mandatory public long-term care insurance.[116][117]
Netherlands
Main articles: Healthcare in the Netherlands and Economic_interventionism § Market-driven_medical_welfare_state
The Netherlands has a dual-level system. All primary and curative care (family doctors, hospitals, and clinics) is financed from private compulsory insurance. Long-term care for the elderly, the dying, the long-term mentally ill etc. is covered by social insurance funded by public spending. According to the WHO, the health care system in the Netherlands was 62% government-funded and 38% privately funded as of 2004.[57]
Insurance companies must offer a core universal insurance package for universal primary, curative care, including the cost of all prescription medicines. They must do this at a fixed price for all. People pay the same premium whether young or old, healthy or sick. It is illegal in The Netherlands for insurers to refuse an application for health insurance, to impose special conditions (e.g., exclusions, deductibles, co-pays etc.), or refuse to fund treatments that a doctor has determined are medically necessary. The system is 50% financed from payroll taxes paid by employers to a fund controlled by the Health regulator. The government contributes an additional 5% to the regulator's fund. The remaining 45% is collected as premiums paid by the insured directly to the insurance company. Some employers negotiate bulk deals with health insurers and some even pay the employees' premiums as an employment benefit. The regulator has sight of the claims made by policyholders and therefore can redistribute the funds its holds on the basis of relative claims made by policy holders. Thus insurers with high payouts receive more from the regulator than those with low payouts. Insurance companies have no incentive to deter high-cost individuals from taking insurance and are compensated if they have to pay out more than might be expected. Insurance companies compete with each other on price for the 45% direct premium part of the funding and try to negotiate deals with hospitals to keep costs low. The competition regulator is charged with checking for abuse of dominant market positions and the creation of cartels that act against consumer interests. An insurance regulator ensures that all basic policies have identical coverage rules so that no person is medically disadvantaged by his or her choice of insurer.
Hospitals in the Netherlands are also regulated and inspected but are mostly privately run and not-for-profit, as are many of the insurance companies. Patients can choose where they want to be treated, and have access to information on the internet about the performance and waiting times at each hospital. Patients dissatisfied with their insurer and choice of hospital can cancel at any time but must make a new agreement with another insurer.
Insurance companies can offer additional services at an extra cost over and above the universal system laid down by the regulator, e.g., for dental care. The standard monthly premium for health care paid by individual adults is about €100 per month. Persons with low incomes can get assistance from the government if they cannot afford these payments. Children under 18 are insured by the system at no additional cost to them or their families because the insurance company receives the cost of this from the regulator's fund. There is a fixed yearly deductible of €385 for each adult person, excluding first visits for diagnosis to general physicians.
Norway
Main article: Healthcare in Norway
Norway has a universal public health system paid largely from taxation in the same way as other Scandinavian countries. The Norwegian health care system is government-funded and heavily decentralized. The health care system in Norway is financed primarily through taxes levied by county councils and municipalities. Dental care is included for children until 18 years old, and is covered for adults for some ailments.[118]
Norway regularly comes top or close to the top of worldwide healthcare rankings.
North Macedonia
Main article: Health in North Macedonia
The country inherited a large health infrastructure after independence in 1991 with good well-distributed public health services. Private hospitals were opened and primary care was privatised. Subsequently, both public and private providers have been integrated into one social insurance-funded model managed by the Health Insurance Fund of North Macedonia. The public hospital sector is seen as inefficient and is unpopular with both patients and professional staff. 90% of the population is within 30 minutes of a health service.
Expenditure on healthcare was $851 per head in 2014, 6.5% of GDP.
According to the Euro health consumer index the Macedonian health system made the most remarkable advance of any country in the history of their Index, from 27th to 16th place in 2014, because by implementing a real-time e-Booking system they reduced waiting lists so significantly. From July 2013, any GP can make a booking at any specialist or heavy diagnostic equipment in the country in real-time while the patient is present. They rated Macedonia 16th in Europe in 2015.
The Doctor's Chamber of Macedonia complains that there is a discrepancy between the available funds and the quality of service expected, that facilities are not used efficiently, equipment is outdated and staff are not used effectively.
Portugal
Main article: Health in Portugal
Portugal's National Healthcare Service, known nationally as Serviço Nacional de Saúde (SNS), is a universal and free healthcare service provided nationwide since 1979 and available to both Portuguese and foreign residents. In 2014, Portugal SNS ranked 13th best healthcare service in Europe.[119] The National Medical Emergency Institute (INEM) is the main emergency medical service and can be activated by calling 112.
Romania
Main article: Healthcare in Romania
According to Article 34 of the Constitution of Romania, the state is obliged "to guarantee the protection of healthcare". Romania has a fully universal healthcare system, which covers medical check-ups, surgical interventions, and any postoperative medical care, as well as free or subsidized medicine for a range of diseases. The state is also obliged to fund public hospitals and clinics. Dental care is not funded by the state, although there are public dental clinics in some hospitals, which treat patients free of charge.
Russia
Main article: Healthcare in Russia
In the former Soviet Union, the preferred term was "socialist medicine"; the Russian language has no term to distinguish between "socialist" and "socialized" (other than "public", Rus: obshchestvenniy/общественный, sometimes "collectivized" or "nationalized", Rus: obobshchestvlenniy/обобществленный).[120][121]
Russia in Soviet times (between 1917 and 1991) had a totally socialist model of health care with a centralized, integrated, hierarchically organised government providing free health care to all citizens. Quality of care and access to medications was not equal however and was dependent on the social status of patient. The best care was provided for nomenklatura and their family members, who had been segregated from the rest of population facilities, such as Kremlin hospital.[122] Initially successful at combating infectious diseases, the effectiveness of the socialized model declined with underinvestment. Despite a doubling in the number of hospital beds and doctors per capita between 1950 and 1980, the quality of care began to decline by the early 1980s and medical care and health outcomes were below western standards.
The new mixed economy Russia has switched to a mixed model of health care with private financing and provision running alongside state financing and provision. The OECD reported that unfortunately, none of this has worked out as planned and the reforms have in many respects made the system worse.[123][needs update] The population's health has deteriorated on virtually every measure. The resulting system is overly complex and very inefficient. It has little in common with the model envisaged by the reformers. Although there are more than 300 private insurers and numerous public ones in the market, real competition for patients is rare leaving most patients with little or no effective choice of insurer, and in many places, no choice of health care provider either. The insurance companies have failed to develop as active, informed purchasers of health care services. Most are passive intermediaries, making money by simply channelling funds from regional OMS funds to healthcare providers.
Article 41 of the Constitution of the Russian Federation confirms a citizen's right to state healthcare and medical assistance free of charge.[124] This is achieved through state compulsory medical insurance (OMS), which is funded by an obligatory medical insurance payroll tax and government subsidies.[125][126] It is worth mentioning that Russian citizens never pay taxes for themselves and often don't even know how much taxes they pay, because tax payment process is maintained by companies they are working on.[127] Introduction in 1993 reform of new free market providers in addition to the state-run institutions intended to promote both efficiency and patient choice. A purchaser-provider split helps facilitate the restructuring of care, as resources would migrate to where there was greatest demand, reduce the excess capacity in the hospital sector and stimulate the development of primary care. Russian Prime Minister Vladimir Putin announced a new large-scale health care reform in 2011 and pledged to allocate more than 300 billion rubles ($10 billion) in the next few years to improve health care in the country. As of 2020 the health insurance tax (called deposition to an OMS fund) is 5.1%.[128]
Serbia
Main article: Healthcare in Serbia
The Constitution of the Republic of Serbia states that it is the right of every citizen to seek medical assistance free of charge.[129] This is achieved by mutual contribution to the Compulsory Social Healthcare Fund of RZZO (Republički Zavod za Zdravstveno Osiguranje or National Health Insurance Institution). The amount of contribution depends on the amount of money the person is making.
Spain
Main article: Healthcare in Spain
Spain provides a public universal health care system for all citizens and, under certain conditions, also non-citizens. Healthcare is free except for co-payments for some products and services; it is mostly paid from the Social Security budget. Adult dental care is not covered but for basic extractions or problems that could result in serious stomatological conditions.
Irrespective of the nationality and insurance situation of the patient, the public system always treats medical emergencies until achieving the best possible outcome. If not covered by the Spanish Social Security (i.e., a visiting foreigner), the provider later negotiates payment with the patient or the patient's insurer. If actually unable to pay, it is covered by Social Security on humanitarian grounds unless the patient purposely traveled to Spain to get free healthcare. Obvious unexpected emergencies such as accidental injuries or sudden illness are customarily covered, but those that could be reasonably expected (e.g., arising from a chronic condition or from avoidable risk-taking) are studied on a case-per-case basis.
According to the World Economic Forum and to Bloomberg, Spain has the most efficient health system in Europe, and also ranks at the top worldwide along with Hong Kong, Japan and Singapore.[130][131]
Private health insurance is available for those who prefer it, and recommended for visitors not covered by the Spanish Social Security or a foreign public or private insurer with overseas coverage.
Sweden
Main article: Healthcare in Sweden
Sweden has a universal public health care system paid for through taxation. The Swedish public and private health care systems are funded through taxes levied by the county councils. Government-paid dental care is accessible to those under 23 years old.
Sweden also has a smaller private health care sector, mainly in larger cities or as centers for preventive health care financed by employers.
In recent years the health care system of Sweden has been heavily criticized for not providing the same quality of health care to all Swedish citizens.[132][133][134][135] This was especially brought to light during the COVID-19 pandemic as Swedish media and public health researchers pointed out that Swedish citizens of other ethnicities than Swedish and people living in working class areas were dying from COVID-19 at a significantly higher rate than the rest of the population.[136][137][138]
Switzerland
Main article: Healthcare in Switzerland
Purchasing basic health insurance is mandatory for all persons residing in Switzerland (within three months of taking up residence or being born in the country).[139] Healthcare in Switzerland is universally available and is regulated by the Federal Health Insurance Act of 1994. Supplemental insurance plans are optional. Insurers are required to offer insurance to everyone, regardless of age or medical condition. They are not allowed to make a profit off this basic insurance, but can on supplemental plans.[140]
Turkey
Main article: Healthcare in Turkey
Turkey achieved universal health coverage in 2003.[141]
The Government's Health Transformation Program of 2003 established a common benefit package that covers primary and preventive care, ambulatory and inpatient care, laboratory services, rehabilitation and follow-up services, pharmaceuticals and medical aids and appliances.[141] Payroll taxes of 12.5% of a person's gross income (5% by the employee and 7.5% by the employer) fund 97%[142] of the program. The government provides for the remaining 3% of the cost.[143]
United Kingdom
Main article: Healthcare in the United Kingdom
Each of the countries of the United Kingdom has a National Health Service that provides public healthcare to all UK permanent residents that was originally designed to be free at the point of need and paid for from general taxation; but changes included introducing charging for prescription medicines and dentistry (those below 16 and those on certain benefits may still get free treatment). However, since health is now a devolved matter, considerable differences are developing between the systems in each of the countries for example Northern Ireland, Scotland and Wales abolished prescription charges.[144] Private healthcare companies are free to operate alongside the public system.
England
Main article: Healthcare in England
Norfolk and Norwich University Hospital, a National Health Service hospital.
The National Health Service (NHS), created by the National Health Service Act 1946, has provided the majority of healthcare in England since its launch on July 5, 1948.[citation needed]
The NHS Constitution for England documents, at a high level, the objectives of the NHS, the legal rights and responsibilities of the various parties (patients, staff, NHS trust boards), and the guiding principles that govern the service.[145] The NHS constitution makes it clear that it provides a comprehensive service, available to all irrespective of age, gender, disability, race, sexual orientation, religion, or belief; that access to NHS services is based on clinical need and not an individual's ability to pay; and that care is never refused on unreasonable grounds. Patient choice in terms of doctor, care, treatments, and place of treatment is an important aspect of the NHS's ambition, and in some cases patients can elect for treatment in other European countries at the NHS's expense. Waiting times are low, with most people able to see their primary care doctor on the same day or the following day.[146] Only 36.1% of hospital admissions are from a waiting list, with the remainder being either emergencies admitted immediately or else pre-booked admissions or the like (e.g., child birth).[147] One of the main goals of care management is to ensure that patients do not experience a delay of more than 18 weeks from initial hospital referral to final treatment, inclusive of time for all associated investigative tests and consultations.[148] In 2009, two-thirds of patients were treated in under 12 weeks.[149]
Though centrally funded, the NHS is not managed by a large central bureaucracy. Responsibility is divided among geographical areas through strategic health authorities. Management is distributed even more locally through primary care trusts, hospital trusts—and increasingly to NHS foundation trusts that provide even more decentralized services within the NHS framework, with more decisions left to local people, patients, and staff. The central government office—the Department of Health—is not involved in day-to-day decision making in either the Strategic Health Authorities or the individual local trusts (primarily health, hospital, or ambulance) or the national specialist trusts such as NHS Blood and Transplant. It does lay down general guidelines they must follow. Local trusts are accountable to their local populations, whilst government ministers are accountable to Parliament for the service overall.[citation needed]
The NHS provides, among other things, primary care, in-patient care, long-term healthcare, psychiatric care and treatments, ophthalmology, and dentistry. All treatment is taxpayer-funded with the exception of certain charges for prescriptions, dentistry and ophthalmology (which themselves are free to children, certain students in full-time education, the elderly, the unemployed and those on low incomes). Around 89 percent of NHS prescriptions are obtained free of charge, mostly for children, pensioners, and pregnant women. Others pay a flat rate of £9.00, and others may cap their annual charges by purchasing an NHS Prescription Prepayment Certificate. Private health care has continued parallel to the NHS, paid for largely by private insurance. Private insurance accounts for only 4 percent of health expenditure and covers little more than a tenth of the population.[150] Private insurers in the UK only cover acute care from specialists. They do not cover generalist consultations, pre-existing conditions, medical emergencies, organ transplants, chronic conditions such as diabetes, or conditions such as pregnancy or HIV.[151]
Most NHS general practitioners are private doctors who contract to provide NHS services, but most hospitals are publicly owned and run through NHS trusts. A few NHS medical services (such as "surgicentres") are sub-contracted to private providers[152] as are some non-medical services (such as catering). Some capital projects such as new hospitals have been funded through the Private Finance Initiative, enabling investment without (in the short term) increasing the public sector borrowing requirement, because long-term contractually obligated PFI spending commitments are not counted as government liabilities.[citation needed]
Northern Ireland
Main article: Health and Social Care in Northern Ireland
Health and Social Care in Northern Ireland is the designation of the national public health service in Northern Ireland.
Scotland
Main article: Healthcare in Scotland
The Royal Aberdeen Children's Hospital is a specialist children's hospital within NHS Scotland.
NHS Scotland, created by the National Health Service (Scotland) Act 1947, was also launched on July 5, 1948, although it has always been a separate organization. Since devolution, NHS Scotland has followed the policies and priorities of the Scottish Government, including the phasing out of all prescription charges by 2011. Prescriptions are now free in Scotland for all citizens. All healthcare in Scotland remains free at the point of use.
Wales
Main article: Healthcare in Wales
NHS Wales was originally formed as part of the same NHS structure created by the National Health Service Act 1946 but powers over the NHS in Wales came under the Secretary of State for Wales in 1969,[153] in turn being transferred under devolution to what is now the Welsh Government.
Crown dependencies
Isle of Man
The Isle of Man, a UK Crown dependency, provides universal public health coverage to its residents.[154]
Guernsey/Jersey
The medical care system in the Channel Islands is very similar to that of the UK in that many of the doctors and nurses have been trained from the UK health perspective.
There is universal health care for residents of Jersey.[155]
Healthcare in Guernsey and Alderney is charged for[156] with all primary care provided for on a private basis.[157][158]
There is no universal healthcare for residents of Sark.
North America
The Bahamas, Barbados, Canada, Costa Rica, Cuba, Jamaica, Mexico, Panama, and Trinidad and Tobago all provide some level of universal health coverage.
Bahamas
The Bahamas approved the National Health Insurance Act in August 2016. The legislation establishes a universal health coverage system that begins with universal coverage of primary health care services, and later expands to include a wide set of benefits that includes all specialized care. The system allows for universal coverage of a basic benefits package and for voluntary insurance to be purchased as a top-up policy to cover services or amenities that are not included in the government plan.[159]
Canada
Main article: Health care in Canada
In 1984, the Canada Health Act was passed, which prohibited extra billing by doctors on patients while at the same time billing the public insurance system. In 1999, the prime minister and most premiers reaffirmed in the Social Union Framework Agreement that they are committed to health care that has "comprehensiveness, universality, portability, public administration and accessibility."[160]
The system is for the most part publicly funded, yet most of the services are provided by private enterprises or private corporations,[citation needed] although most hospitals are public. Most doctors do not receive an annual salary, but receive a fee per visit or service.[161] About 29% of Canadians' health care is paid for by the private sector or individuals.[162] This mostly goes towards services not covered or only partially covered by Medicare such as prescription drugs, dentistry, physiotherapy and vision care.[163] Many Canadians have private health insurance, often through their employers, that cover these expenses.[164]
The Canada Health Act of 1984 "does not directly bar private delivery or private insurance for publicly insured services," but provides financial disincentives for doing so. "Although there are laws prohibiting or curtailing private health care in some provinces, they can be changed," according to a report in the New England Journal of Medicine.[165][166] The legality of the ban was considered in a decision of the Supreme Court of Canada, which ruled in Chaoulli v. Quebec that "the prohibition on obtaining private health insurance, while it might be constitutional in circumstances where health care services are reasonable as to both quality and timeliness, is not constitutional where the public system fails to deliver reasonable services." The appellant contended that waiting times in Quebec violated a right to life and security in the Quebec Charter of Human Rights and Freedoms. The Court agreed, but acknowledged the importance and validity of the Canada Health Act, and at least four of the seven judges explicitly recognized the right of governments to enact laws and policies that favour the public over the private system and preserve the integrity of the public system.
Costa Rica
Universal healthcare and pensions are run by the Caja Costarricense de Seguro Social (CCSS). In 1941, Costa Rica established Caja Costarricense de Seguro Social (CCSS), a social security insurance system for wage-earning workers. In 1961, coverage was expanded to include workers' dependents and from 1961 to 1975, a series of expansions extended coverage for primary care and outpatient and inpatient specialized services to people in rural areas, the low-income population, and certain vulnerable populations. Further expansions during the late 1970s extended insurance coverage to farmers, peasants, and independent contract workers. Additionally, CCSS mandates free health service provision to mothers, children, indigenous people, the elderly, and people living with disabilities, regardless of insurance coverage. By 2000, 82 percent of the population was eligible for CCSS, which has continued to expand in the ensuing period. By covering all population groups through the same system, Costa Rica has avoided social insurance stratification and inequity common in many other countries in the region.[167]
CCSS is funded by a 15 percent payroll tax, as well as payments from retiree pensions [6]. Taxes on luxury goods, alcohol, soda, and imported products also help to cover poor households who do otherwise pay into the system. All CCSS funds are merged into a single pool, which is managed by the central financial administration of CCSS. In 1973, the Ministry of Health decided to move away from direct service provision and adopt a steering role. Responsibility for the provision of most care was transferred to the CCSS, although the Ministry retained responsibility for disease control, food and drug regulation, environmental sanitation, child nutrition, and primary care for the poor. Through the CCSS, health care is now essentially free to nearly all Costa Ricans. Private health care is also widely available and INS offers private health insurance plans to supplement CCSS insurance.[168]
Cuba
Main article: Healthcare in Cuba
The Cuban government operates a national health system and assumes fiscal and administrative responsibility for the health care of all its citizens. There are no private hospitals or clinics as all health services are government-run. All healthcare in Cuba is free to Cuban residents.[169] The present Minister for Public Health is Roberto Morales Ojeda. The Cuban government sends doctors and other medical personnel overseas as part of medical missions. These missions are mainly in Latin America, Africa, and Oceania and have had substantial positive impacts on the local populations served. Cuba also brings medical students and patients to Cuba for training and treatment respectively.
Mexico
Main article: Healthcare in Mexico
Public health care became universal healthcare on January 1, 2020,[170] mandated by the new President Andrés Manuel López Obrador and approved by Congress. It is completely free for Mexican citizens who do not have health insurance. Mexico's new universal healthcare, administered by the Instituto de Salud para el Bienestar (Institute of Health for Welfare, INSABI), includes free consultations with family doctors and specialists, free medications, free surgeries, free dental and vision[citation needed]. As of 2020, public health care is provided to all Mexican citizens as guaranteed via Article 4 of the Constitution. Public care is now fully subsidized by the federal government. All Mexican citizens are eligible for subsidized health care regardless of their work status via a system of health care facilities operating under the federal Secretariat of Health (formerly the Secretaria de Salubridad y Asistencia, or SSA) agency.
Employed citizens and their dependents, however, are further eligible to use the health care program administered and operated by the Instituto Mexicano del Seguro Social (IMSS) (English: Mexican Social Security Institute). The IMSS health care program is a tripartite system funded equally by the employee, its private employer, and the federal government. The IMSS does not provide service to employees of the public sector. Employees in the public sector are serviced by the Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado (ISSSTE) (English: Institute for Social Security and Services for State Workers), which attends to the health and social care needs of government employees. This includes local, state, and federal government employees. The government of the states in Mexico also provide health services independently of those services provided by the federal government programs. In most states, the state government has established free or subsidized healthcare for all their citizens.
In 2006, the Mexican government created the Health Insurance for a New Generation also known as "life insurance for babies".[171][172][173] On May 28, 2009, Universal Care Coverage for Pregnant Women was introduced.[174] In a 2020 expansion of health care coverage, all Mexicans are now covered.
Trinidad and Tobago
Main article: Healthcare in Trinidad and Tobago
A universal health care system is used in Trinidad and Tobago and is the primary form of health care available in the country. It is used by the majority of the population seeking medical assistance, as it is free for all citizens. Responsibility for the provision of healthcare services in Trinidad and Tobago was devolved from the Ministry of Health to Regional Health Authorities under the Regional Health Authorities Act No. 5 in 1994.
United States
Main article: Healthcare in the United States
Between 2010 and 2019, the individual shared responsibility provision of the Affordable Care Act required Americans, with certain exemptions, to have private or public health insurance.[175] Otherwise, they were required to pay a fine.
South America
Argentina, Brazil, Chile, Colombia, Ecuador, Peru, Uruguay, and Venezuela all provide some level of universal health coverage.
Argentina
Main article: Health care in Argentina
Health care is provided through a combination of employer and labor union-sponsored plans (Obras Sociales), government insurance plans, public hospitals and clinics and through private health insurance plans. It costs almost 10% of GDP and is available to anyone regardless of ideology, beliefs, race or nationality.
Brazil
Main article: Healthcare in Brazil
The universal health care system was adopted in Brazil in 1988 after the end of the military dictatorship. However, universal health care was available many years before, in some cities, once the 27th amendment to the 1969 Constitution imposed the duty of applying 6% of their income in healthcare on the municipalities.[176] The Brazilian universal health care is called SUS (Sistema Único de Saúde), which covers all treatments, surgeries and medications for all resident and non-resident individuals within Brazilian jurisdiction, regardless of ethnicity, nationality, or visa - including tourists, passengers in transit and refugees.
Chile
Main article: Healthcare in Chile
Health care in Chile is provided by the government (via public corporation FONASA, National Healthcare Fund) and by private insurers (via ISAPRE, Previsional Healthcare Institutions). All workers and pensioners are mandated to pay 7% of their income for health care insurance (the poorest pensioners are exempt from this payment but medications are expensive and pensioners have to pay). Workers who choose not to join an Isapre, are automatically covered by Fonasa. Fonasa also covers unemployed people receiving unemployment benefits, uninsured pregnant women, insured worker's dependant family, people with mental or physical disabilities and people who are considered poor or indigent.
Fonasa costs vary depending on income, disability or age. Attention at public health facilities via Fonasa is free for low-income earners, people with mental or physical disabilities and people over the age of 60. Others pay 10% or 20% of the costs, depending on income and the number of dependants. Fonasa beneficiaries may also seek attention in the private sector, for a designated fee.
Additionally, exist the GES Plan (Explicit Guarantees in Healthcare Plan), that consists of a defined number of high-morbility and mortality diseases (currently 85) that have special mandatory attention guarantees for all people, both Isapre and Fonasa affiliates, in relation to:
Access: Universal access to treatment if required. Individuals will be able to get attention from a provider near their place of residence.
Opportunity: Opportune waiting times, there is a maximum pre-established time limit to get initial and post-diagnosis attention.
Financial protection: Law-fixed maximum price with low copayments to providers (maximum copayment of 20% of the cost), the payment cannot be an obstacle to attention. The total cost must not exceed one monthly income for the family in a year.
Best possible quality of service: Attention only in accredited public or private Health centers, that follow technical requirement standards that will be established based on medical evidence.
The treatment protocols and number of diseases included are evaluated every 3 years by the authorities.
Colombia
Main article: Health care in Colombia
In 1993 a reform transformed the health care system in Colombia, trying to provide a better, sustainable, health care system and to reach every Colombian citizen.
Peru
Main article: Healthcare in Peru
On April 10, 2009, the Government of Peru published the Law on Health Insurance to enable all Peruvians to access quality health services, and contribute to regulating the financing and supervision of these services. The law enables all population to access diverse health services to prevent illnesses, and promote and rehabilitate people, under a Health Basic Plan (PEAS).[177][178]
On April 2, 2010, President Alan Garcia Perez signed a supreme ordinance approving the regulations for the framework law on Universal Health Insurance, which seeks to provide access to quality health care for all Peruvian citizens.
Peru's Universal Health Insurance law aims to increase access to timely and quality health care services, emphasizes maternal and child health promotion, and provides the poor with protection from financial ruin due to illness.[179]
The regulation states that membership of the Universal Health Insurance (AUS for its Spanish acronym) is compulsory for the entire population living in the country. To that end, the Ministry of Health will approve, by supreme ordinance, the mechanisms leading to compulsory membership, as well as escalation and implementation.[180]
Suriname
Main article: Health in Suriname
The National Basic Health Insurance Law, introduced in 2014, provides access to a basic package of primary, secondary, and tertiary care services for citizens. It repeals the Healthcare Tariffs Law from 2005.
Uruguay
Main article: Health in Uruguay
Public health insurance is available, but not mandatory, to all residents.
Oceania
Australia and New Zealand both have universal health care. Hospitalisation is free for permanent residents in both nations. In addition, Australia grants primary care coverage, while in New Zealand general practice and prescriptions are subsidised only.
Australia
Main articles: Medicare (Australia) and Health care in Australia
In Australia, Medibank—as it was then known—was introduced, by the Whitlam Labor government on July 1, 1975, through the Health Insurance Act 1973. The Australian Senate rejected the changes multiple times and they were passed only after a joint sitting after the 1974 double dissolution election. However, Medibank was supported by the subsequent Fraser Coalition (Australia) government and became a key feature of Australia's public policy landscape. The exact structure of Medibank/Medicare, in terms of the size of the rebate to doctors and hospitals and the way it has administered, has varied over the years. The original Medibank program proposed a 1.35% levy (with low-income exemptions) but these bills were rejected by the Senate, so Medibank was funded from general taxation. In 1976, the Fraser Government introduced a 2.5% levy and split Medibank in two: a universal scheme called Medibank Public and a government-owned private health insurance company, Medibank Private.
In 1984, Medibank Public was renamed Medicare by the Hawke Labor government, which also changed the funding model, to an income tax surcharge, known as the Medicare Levy, which was set at 1.5%, with exemptions for low-income earners.[181] The Howard Coalition government introduced an additional levy of 1.0%, known as the Medicare Levy Surcharge, for those on high annual incomes ($70,000) who do not have adequate levels of private hospital coverage.[182] This was part of an effort by the Coalition to encourage take-up of private health insurance. According to WHO, government funding covered 67.5% of Australia's health care expenditures in 2004; private sources covered the remaining 32.5% of expenditures.[57]
As of 2019, the Medicare levy is 2% of taxable income,[183] with a Medicare levy surcharge, for those on high income who do not have appropriate private patient hospital cover (1% for singles on $90,000 pa and families on $180,000 pa, rising to 1.5% for higher incomes).[184]
In addition to Medicare, there is a separate Pharmaceutical Benefits Scheme, funded by the federal government, which substantially subsidises a range of prescription medications.
New Zealand
Main article: Health care in New Zealand
As with Australia, New Zealand's healthcare system is funded through general taxation according to the Social Security Act 1938. However, aside from hospitalisation, there are user charges for prescriptions (introduced in February 1985, (this ended in mid 2023 when funded drugs became free under prescription)) and partial subsidisation of general practitioner visits with additional provision for those on low or modest incomes known as Community Service Cards (introduced on February 1, 1992) to target healthcare based on income.[185][186][187] These changes were part of broader controversial policies introduced by the Fourth National Government between 1991 and 1993 and effectively ended largely free provision of primary healthcare. According to the WHO, government sources covered 77.4% of New Zealand's health care costs in 2004; private expenditures covered the remaining 22.6%.
Historic attempts to bring general practitioner care into government ownership have been largely unfulfilled.
There are twenty district health boards as of 2019 whose task is ensuring the provision of health and disability services to populations within a defined geographical area and are partially elected while the remainder is appointed by New Zealand's Minister of Health.[188] This system of management came into being on January 1, 2001, abolishing the much controversial Crown Health Enterprises regime which had replaced Area Health Boards previously.
https://en.wikipedia.org/wiki/List_of_c ... ealth_care
Cual es el problema de dar salud a los mayores de 65 años cuando es evidentemente mas costoso que vayan a salas de emergencia, o prefieren que se mueran por no poder pagar una consulta o una medicina?
Que clase de gente son algunos de los que escriben por aca?
Increible.
List of countries with universal health care
From Wikipedia, the free encyclopedia
Government-guaranteed health care for all citizens of a country, sometimes called universal health care, is a broad concept that has been implemented in several ways. The common denominator for all such programs is some form of government action aimed at broadly extending access to health care and setting minimum standards. Most implement universal health care through legislation, regulation, and taxation. Legislation and regulation direct what care must be provided, to whom, and on what basis.
The logistics of such health care systems vary by country. Some programs are paid for entirely out of tax revenues. In others, tax revenues are used either to fund insurance for the very poor or for those needing long-term chronic care. In some cases such as the UK, government involvement also includes directly managing the health care system, but many countries use mixed public-private systems to deliver universal health care. Alternatively, much of the provision of care can be contracted from the private sector, as in the case of Canada and France. In some instances, such as in Italy and Spain, both these realities may exist at the same time. The government may provide universal health insurance in the form of a social insurance plan that is affordable by all citizens, such as in the case of Germany and Taiwan, although private insurance may provide supplemental coverage to the public health plan. In twenty-five European countries, universal healthcare entails a government-regulated network of private insurance companies.[1][2]
As of 2021, Brazil is the only country where any individual within the state's jurisdiction is eligible to receive free healthcare with no previous application, which covers all treatments, surgeries, and medications at any condition, whether resident or non-resident, regardless of ethnicity, nationality, or visa, including tourists, passengers in transit, and refugees.[3]
Africa
Algeria
Algeria operates a public healthcare system. It is a universal healthcare system as well. A network of hospitals, clinics, and dispensaries provide treatment to the population, with the Social Security system funding health services, although many people must still cover part of their costs due to the rates paid by the Social Security system remaining unchanged since 1987. The poor are generally entitled to taxpayer funded health services, while the wealthy pay for treatment according to a sliding scale.[4][5]
Botswana
Main article: Health in Botswana
Botswana established a free healthcare system that operates a system of public medical centers, with 98% of health facilities in the country run by the government.[citation needed] All citizens are entitled to be treated in taxpayer funded facilities, though a nominal fee of ~70 BWP (~US$6.60) is typically charged for public health services except for sexual reproductive health services and antiretroviral therapy services, which are free.[6]
Burkina Faso
Burkina Faso provides universal healthcare to citizens through a system called Universal Health Insurance (AMU)—administered by two bodies, one for civilians and the other for the armed forces.[7]
Mauritius
The Government of Mauritius operates a system of medical facilities that provide treatment to citizens free of charge.[8]
Morocco
Morocco does not have universal health care. It is currently building a system which was slated to cover the entire population by the end of 2022.[9] The country operates a public health sector run by the government that operates 85% of the country's hospital beds. It deals mainly with the poor and rural populations, who cannot afford private healthcare. In addition, a non-profit health sector operated by the National Social Security Fund covers 16% of the population. Private medical care is available for those who can afford it.[10]
Rwanda
Main article: Healthcare in Rwanda
Rwanda operates a system of universal health insurance through the Ministry of Health called Mutuelle de Santé (Mutual Health), a system of community-based insurance where people pay premiums based on their income level into local health insurance funds, with the wealthiest paying the highest premiums and required to cover a small percentage of their medical expenses, while those at the lowest income levels are exempt from paying premiums and can still utilize the services of their local health fund. In 2012, this system insured all but 4% of the population.[11]
Seychelles
The government of Seychelles operates a system of medical facilities that provide treatment to citizens free of charge.
Tunisia
Tunisia operates a public healthcare system under the National Health Insurance Fund (Caisse Nationale d'Assurance Maladie). All Tunisian citizens and residents can receive treatment in state-run hospitals and clinics for a very low co-pay, while people with the lowest income are able to apply for an exemption from co-pays.[12]
Asia
Countries and regions that provide public healthcare in Asia include Bangladesh, Bhutan,[13] Bahrain,[14] Brunei, China, Hong Kong, India, Indonesia,[15] Iran,[16] Israel[17] (see below), Jordan,[18] Kazakhstan,[19] Macau (see below), Malaysia,[20] Mongolia,[21] Oman,[22] Pakistan (KPK),[23] Philippines,[24] Singapore, Qatar, DPRK (North Korea),[25] Sri Lanka,[26] Syria,[27] Taiwan (R.O.C.)[28] (see below), Japan, South Korea, and Saudi Arabia.
Bhutan
Main article: Health in Bhutan
The Royal Government of Bhutan maintains a policy of free and universal access to primary health care. As hospital facilities in the country are limited, patients with diseases that cannot be treated in Bhutan, such as cancer, are normally referred to hospitals in India for treatment. Such referral treatment is also carried out at the cost of the Royal Government.[29]
China
Main article: Healthcare reform in China
As of 2017, more than 97% of people in China are covered by one of three categories of public health insurance. From most generous to least generous, they are the:
Urban Employee Basic Medical Insurance (UEBMI, 职工医保)
Urban Resident Basic Medical Insurance (URBMI, 居民医保)
New Cooperative Medical Service (NCMS, 新农合)
The UEBMI is funded by 6-12% by employers and 2% by employees; the URBMI entirely by local governments, and it covers students, the unemployed, and the retired; and the NCMS by the central government. In 2016, the government announced plans to merge NCMS with URBMI. China also has five private health insurance companies for supplementary care: the three largest are Ping An, PICC, and China Life. [30] For the public plans, the list of covered procedures is limited, and copayment is common. The proportion of out-of-pocket costs depends on profession and location: for example, workers in urban Shanghai might have 85% of their medical costs covered up to $740,000 while workers in rural Guiyang are reimbursed for 65% of their medical costs up to $29,000 annually.[31]
Immediately after the Chinese Communist Revolution in 1949, the state both directly operated all hospitals and clinics. The government paid for healthcare services, and life expectancy improved greatly, although the services provided were basic. State-provided health insurance varied by area: the Cooperative Medical System (CMS) covered rural areas, while the Government Insurance Scheme (GIS) and Labor Insurance Scheme (LIS) covered residents of urban areas.[32] After the Chinese economic reform in 1978, the state reduced spending on hospitals and allowed them to charge patients for profit. The state, however, did not stop paying for certain healthcare services like mandatory vaccination.[31]
From the high point of privatization of healthcare in the 1990s,[32] China has been reforming with universal health care as a goal in the 21st century, as part of the "moderately prosperous society" plan. The New Rural Co-operative Medical Care System (NRCMCS) from 2005, aimed at the rural poor, sets the annual cost of medical coverage at 50 yuan (US$7) per person. As of September 2007, around 80% of the whole rural population of China had signed up (about 685 million people). For patients who go to a small hospital or clinic in their local town, the scheme covers from 70 to 80% of their bill; patients at a county provider get 60% of their cost covered; and in a large modern city hospital, the scheme covers about 30% of the bill.[33]
At the end of 2008, the government published its reform plan clarifying government's responsibility by saying that it would play a dominant role in providing public health and basic medical service. The plan listed public health, rural areas, city community health services and basic medical insurance as four key areas for government investment. It also promised to tighten government control over medical fees in public hospitals and to set up a "basic medicine system" to cover drug costs.[34][35] China's "Law on Promotion of Basic Medical and Health Care", effective June 2020, asserts that Chinese citizens have a positive right to healthcare, regardless of cost. Additional laws are expected to specify what this right will mean in practice.[citation needed]
Hong Kong
Main article: Health in Hong Kong
Hong Kong has early health education, professional health services, and well-developed health care and medication system. The life expectancy is 84 for females and 78 for males,[36] which is the second highest in the world, and 2.94 infant mortality rate, the fourth lowest in the world.[37][38]
There are two medical schools in Hong Kong, and several schools offering courses in traditional Chinese medicine. The Hospital Authority is a statutory body that operates and manages all public hospitals. Hong Kong has high standards of medical practice. It has contributed to the development of liver transplantation, being the first in the world to carry out an adult to adult live donor liver transplant in 1993.[39]
India
Main article: Healthcare in India
At the federal level, a national health insurance program was launched in 2018 by the Government of India, called Ayushman Bharat. This aimed to cover the bottom 50% (500 million people) of the country's population working in the unorganized sector (enterprises having less than 10 employees) and offers them free treatment at both public and private hospitals.[40] For people working in the organized sector (enterprises with more than 10 employees) and earning a monthly salary of up to Rs 21000 are covered by the social insurance scheme of Employees' State Insurance which entirely funds their healthcare (along with pension and unemployment benefits), both in public and private hospitals.[41][42] People earning more than that amount are provided health insurance coverage by their employers through the many public or private insurance companies. As of 2020, 300 million Indians are covered by insurance bought from one of the public or private insurance companies by their employers as group or individual plans.[43] Unemployed people without coverage are covered by the various state insurance schemes if they do not have the means to pay for it.[44] In 2019, the total net government spending on healthcare was $36 billion or 1.23% of its GDP.[45] An outpatient card at AIIMS costs a one-time fee of 10 rupees (around 20 cents U.S.) and thereafter outpatient medical advice is free. In-hospital treatment costs is extremely minimal and depends on the financial condition of the patient and the facilities utilized, but are usually much less than in the private sector. For instance, a patient is waived treatment costs if their income is below the poverty line. However, getting treatment at high quality government hospitals is very tough due to the high number of people needing healthcare and the lack of sufficient facilities.
Primary health care is provided by city and district hospitals and rural primary health centres (PHCs). These hospitals provide treatment free of cost. Primary care is focused on immunization, prevention of malnutrition, pregnancy, child birth, postnatal care, and treatment of common illnesses.[46] Patients who receive specialized care or have complicated illnesses are referred to secondary (often located in district and taluk headquarters) and tertiary care hospitals (located in district and state headquarters or those that are teaching hospitals).[citation needed]. In urban cities and towns like Delhi, there are neighbourhood health clinics called Mohalla Clinics which offer completely free treatment, testing and drugs.[47]
The Indian government has launched Ayushyaman Bharat Yojana (AB-NHPM), which will provide all Indian citizens with insurance coverage for serious illnesses, and free drugs and diagnostic treatments.[48]
Indonesia
Main article: Healthcare in Indonesia
Indonesia is currently building a universal healthcare system with its Jaminan Kesehatan Nasional (JKN) scheme, managed by BPJS Kesehatan, which covers a range of treatments from public providers as well as private providers that opt to participate. The scheme is funded by premiums from the employed. The formally employed pay a premium worth 5% of their salary, with 1% paid by the employee and 4% paid by the employer, while informal workers and the self-employed must pay a fixed monthly premium. As of April 2018, 75% of the population was covered by JKN.[49]
While the country has a number of government-owned hospitals, about 63% are privately owned.[50] Indonesia also operates a three-tier community health system. The Ministry of Health oversees a network of Puskesmas, or community health centers, followed by health sub-centers and village-level integrated posts.[51]
Israel
Main article: Healthcare in Israel
Health care in Israel as a percentage of GDP
Israel has a system of universal healthcare as set out by the 1995 National Health Insurance Law. The state is responsible for providing health services to all residents of the country, who can register with one of the four national health service funds. To be eligible, a citizen must pay a health insurance tax. Coverage includes medical diagnosis and treatment, preventive medicine, hospitalization (general, maternity, psychiatric and chronic), surgery and transplants, preventive dental care for children, first aid and transportation to a hospital or clinic, medical services at the workplace, treatment for drug abuse and alcoholism, medical equipment and appliances, obstetrics and fertility treatment, medication, treatment of chronic diseases and paramedical services such as physiotherapy and occupational therapy.[52]
In Israel, the National Health Insurance Law is the legal framework that enables and facilitates basic, compulsory universal health care. Promoted by health minister Haim Ramon in the early 1990s,[53] the Knesset put the law into effect on January 1, 1995—basing it on recommendations from a National Committee of Inquiry headed by Shoshana Netanyahu, which examined restructuring the health care system in Israel in the late 1980s. Prior to the law's passage, over 90% of the population was already covered by voluntarily belonging to one of four nationwide, not-for-profit sickness funds. These operated some of their own medical facilities, funded in part by employers and the government, and in part by the insured via levies that varied according to income. However, there were three problems associated with this arrangement. First, membership in the largest fund, Clalit, required one to belong to the Histadrut labor organization, even if a person did not want to (or could not) have such an affiliation, and other funds restricted entry to new members based on age, pre-existing conditions, or other factors. Second, different funds provided different levels of benefit coverage or services to their members. Lastly, some of the population, albeit a small percentage, had no health insurance.
Before the law went into effect, all the funds collected premiums directly from members. However, upon passage of the law, a new progressive national health insurance tax was levied through Bituah Leumi (Israel's social security agency), which then re-distributes the proceeds to the sickness funds based on their membership and its demographic makeup. This ensured that all citizens would now have health coverage. While membership in one of the funds now became compulsory for all, free choice was introduced into movement of members between funds (a change is allowed once every six months), effectively making the various sickness funds compete equally for members among the populace. Annually, a committee appointed by the ministry of health publishes a "basket" or uniform package of medical services and prescription formulary that all funds must provide as a minimum to all members. Achieving this level of equality guaranteed basic healthcare regardless of fund affiliation, which was one of the principal aims of the law. An appeals process handles rejection of treatments and procedures by the funds and evaluates cases that fall outside the "basket" of services or prescription formulary.
The law is generally considered a success, and Israeli citizens enjoy a high standard of medical care comparatively, with more competition in the country's health care, and with order having brought to what was once a somewhat disorganized system—the law nevertheless has its critics. First among the criticisms is that the "basket" may not provide enough coverage. To partly address this, the health funds began offering "supplementary" insurance to cover certain additional services not in the basket. However, since this insurance is optional (though rather modestly priced, costing the equivalent of about US$10 to $35 a month depending on age and coverage for an adult in 2019), critics argue that it goes against the spirit of the new law, which stressed equality of healthcare for all citizens. Another criticism is that, to provide universal coverage to all, the tax income base amount (the maximum amount of yearly earnings that are subject to the tax) was set rather high, causing many high-income taxpayers to see the amount they pay for their health premiums (now health tax) skyrocket. Finally, some complain about the constantly rising costs of copayments for certain services.
Japan
Main article: Health care system in Japan
All residents of Japan are required by the law to have health insurance coverage. People without insurance from employers can participate in a national health insurance programme, administered by local governments. Patients are free to select physicians or facilities of their choice and cannot be denied coverage. Hospitals, by law, must be run as non-profit and be managed by physicians.
Kuwait
Main article: Healthcare in Kuwait
Kuwait offers universal healthcare.
Macau
Main article: Healthcare in Macau
Macau offers universally accessible single-payer system funded by taxes. Health care is provided by the Health Bureau.
Malaysia
Malaysia has achieved universal health coverage. It has made remarkable progress in improving health outcomes over the past seven decades. At the time of Independence, the number of infant deaths was 75.5 per 1,000 live births. This has since fallen by more than 90 percent to 6.7 deaths per 1,000 live births in 2016. Maternal mortality which refers to the death of a woman caused by her pregnancy, during and after delivery, has also decreased by 89% between 1963 and 2013.[54]
Maldives
Aasandha is the national healthcare insurance scheme of the Maldives. It provides taxpayer-funded medical assistance to all Maldivian citizens. National Social Protection Agency of Maldives was formed under the National Social Health Insurance Act on August 27, 2008. It is mandated to administer the National Social Health Insurance Scheme and by an executive order under the same act mandated to conduct social protection programs identified by the government of Maldives. NSPA is also the responsible agency to regulate and conduct Social Protection programs under the Social Protection Act.
Pakistan
In Pakistan, Universal Healthcare exists on provincial levels, started by the Government of Khyber Pakhtunkhwa, which had launched a "universal health insurance programme" known as the "Sehat Insaf Card" to provide free healthcare for the residence of KPK, where families would be covered up to Rs. 10 lakh (US$3,500) for treatment.[23] This was further expanded to the Punjab province of Pakistan, in December 2021, to cover more than 31 million families. Prime Minister Imran Khan announced that an additional Rs. 440 billion (US$1.5 billion) would be spent to cover the entire province.[55]
Philippines
Filipinos are covered under the National Health Insurance Program (NHIP) of the Philippine government-owned Philippine Health Insurance Corporation or PhilHealth. Under the Universal Health Care Law of 2019, all Filipinos were automatically enrolled in the NHIP.[56]
Saudi Arabia
The Government of Saudi Arabia provides free universal health coverage for all citizens. Non-citizens are required by law to have private insurance paid for by their employer.
Singapore
Main article: Healthcare in Singapore
Singapore has a universal health care system where government ensures affordability, largely through compulsory savings and price controls, while the private sector provides most care. Overall spending on health care amounts to only 3% of annual GDP. Of that, 66% comes from private sources.[57] Singapore currently has the second lowest infant mortality rate in the world and among the highest life expectancies from birth, according to the World Health Organization.[58] Singapore has "one of the most successful healthcare systems in the world, in terms of both efficiency in financing and the results achieved in community health outcomes," according to an analysis by global consulting firm Watson Wyatt.[59] Singapore's system uses a combination of compulsory savings from payroll deductions (funded by both employers and workers) a nationalized health insurance plan, and government subsidies, as well as "actively regulating the supply and prices of healthcare services in the country" to keep costs in check; the specific features have been described as potentially a "very difficult system to replicate in many other countries." Many Singaporeans also have supplemental private health insurance (often provided by employers) for services not covered by the government's programs.[59]
South Korea
Main article: Healthcare in South Korea
South Koreans have access to a universal healthcare safety net, although a significant portion of healthcare is privately funded.
North Korea
Main article: Health in North Korea
North Korea claims to provide universal health care with a national medical service and health insurance system.[60] It claims that health services are offered for free.[60]: 7–8 However, this claim has been contrasted by North Korean defectors, who claim that patients must in fact pay for health services, that the upper classes have access to a higher standard of healthcare than ordinary ones do, and that "how much money a patient has determines whether they live or die".[61]
Sri Lanka
Main article: Healthcare in Sri Lanka
Sri Lanka provides free universal healthcare to their citizens.[62]
Taiwan
Main article: Healthcare in Taiwan
The current health care system in Taiwan, known as National Health Insurance (NHI), was instituted in 1995. NHI is a single-payer compulsory social insurance plan that centralizes the disbursement of health care dollars. The system promises equal access to health care for all citizens, and the population coverage had reached 99% by the end of 2004.[63] NHI is mainly financed through premiums based on the payroll tax, and is supplemented with out-of-pocket payments and direct government funding. In the initial stage, fee-for-service predominated for both public and private providers.[citation needed]
NHI delivers universal coverage offered by a government-run insurer. The working population pays premiums split with their employers, others pay a flat rate with government help and the poor or veterans are fully subsidized.[64]
Under this model, citizens have free range to choose hospitals and physicians without using a gatekeeper and do not have to worry about waiting lists. NHI offers a comprehensive benefit package that covers preventive medical services, prescription drugs, dental services, Chinese medicine, home nurse visits and many more. Since NHI, the previously uninsured have increased their usage of medical services. Most preventive services are free such as annual checkups and maternal and child care. Regular office visits have co-payments as low as US$5 per visit. Co-payments are fixed and unvaried by the person's income.[65]
Thailand
Main article: Healthcare in Thailand
Thailand introduced universal coverage reforms in 2001, becoming one of only a handful of lower-middle income countries to do so at the time. Means-tested health care for low income households was replaced by a new and more comprehensive insurance scheme, originally known as the 30 baht project, in line with the small co-payment charged for treatment. People joining the scheme receive a gold card that they use to access services in their health district, and, if necessary, get referrals for specialist treatment elsewhere. The bulk of finance comes from public revenues, with funding allocated to Contracting Units for Primary Care annually on a population basis. According to the WHO, 65% of Thailand's health care expenditure in 2004 came from the government, and 35% was from private sources.[57] Although the reforms have received a good deal of critical comment, they have proved popular with poorer Thais, especially in rural areas, and survived the change of government after the 2006 military coup. The then Public Health Minister, Mongkol Na Songkhla, abolished the 30 baht co-payment and made the UC scheme free. It is not yet clear whether the scheme will be modified further under the coalition government that came to power in January 2008.[66][67][68]
In 2016, Thailand became the first country in Asia to eliminate HIV transmission from mother to child, owing to its robust public healthcare system.[69]
United Arab Emirates
Main article: Healthcare in the United Arab Emirates
The United Arab Emirates has enacted federal legislation that requires universal healthcare nationals and mandatory health insurance for expatriates, but this legislation has not yet been implemented across the entire country. [70]
Europe
Main article: Healthcare in Europe
Almost all European countries have healthcare available for all citizens. Most European countries have systems of competing private health insurance companies, along with government regulation and subsidies for citizens who cannot afford health insurance premiums.[71] Countries with universal healthcare include Austria, Belarus,[72] Bulgaria, Croatia, Czech Republic, Denmark, Finland, France, Germany, Greece, Iceland, Italy, Latvia, Lithuania, Luxembourg, Macedonia, Malta, Moldova,[73] Norway, Poland, Portugal,[74] Romania, Russia, Serbia, Spain, Sweden, Switzerland, Ukraine,[75] and the United Kingdom.[76]
Albania
Main article: Healthcare in Albania
Healthcare in Albania is universal for citizens of Albania.
Armenia
Main article: Healthcare in Armenia
Armenia operates a mandatory social health insurance system. The majority of the population is enrolled in the Compulsory Health Insurance Fund, which is funded through payroll taxes and contributions from employers and employees.
Austria
Main article: Healthcare in Austria
Healthcare in Austria is universal for residents of Austria as well as those from other EU countries.[77] Austria has a two-tier payment system in which many individuals receive basic publicly funded care; they also have the option to purchase supplementary private health insurance.
Belgium
Main article: Healthcare in Belgium
Healthcare in Belgium is composed of three parts. Firstly there is a primarily publicly funded healthcare and social security service run by the federal government, which organises and regulates healthcare; independent private/public practitioners, university/semi-private hospitals and care institutions. There are a few (commercially run for-profit) private hospitals.[78] Secondly is the insurance coverage provided for patients. Finally, industry coverage covers the production and distribution of healthcare products for research and development. The primary aspect of this research is done in universities and hospitals.
Bulgaria
Healthcare in Bulgaria is mixed. Some services are private, like dental care, and some services are run publicly by NHIF.[79] Because 15% of the population is uninsured and cannot access most health services, it does not currently qualify as having universal healthcare.[80]
Croatia
Main article: Healthcare in Croatia
Croatia has a universal health care system that provides medical services and is coordinated by the Ministry of Health. The population is covered by a basic health insurance plan provided by statute and by optional insurance. It is administered by the Croatian Health Insurance Fund. In 2012, annual compulsory healthcare related expenditures reached 21.0 billion kunas (c. 2.8 billion euro). There are hundreds of healthcare institutions in Croatia, including 79 hospitals and clinics with 25,285 beds, caring for more than 760 thousand patients per year, 5,792 private practice offices and 79 emergency medical service units.
Cyprus
Main article: Health care in Cyprus
A universal national health system, known as GESY, was implemented in Cyprus in June 2019. The new system aims to provide affordable and effective medical care to all people residing permanently in Cyprus. As of June 2022, 917,000 Cypriots have registered[5][clarification needed] with a general practitioner through the GESY system, which is roughly the current population of the Republic of Cyprus.
Czech Republic
Main article: Healthcare in the Czech Republic
Czech Republic has a universal public health system paid largely from taxation. Private health care systems do co-exist freely alongside public ones, sometimes offering better quality or faster service. Almost all medical services are covered by health insurance and insurance companies, though certain services such as prescription drugs or vision and dental care are only covered partially.
Denmark
Main article: Health care in Denmark
Denmark has a universal public health system paid largely from taxation with local municipalities delivering health care services in the same way as other Scandinavian countries. Primary care is provided by a general practitioner service run by private doctors contracting with the local regions with payment on a mixed per capita and fee for service basis. Most hospitals are run by the regions (only 1% of hospital beds are in the private sector).
Estonia
Main article: Healthcare in Estonia
Estonia's health care system is based on compulsory insurance based on solidarity funding and on universal access to services provided by private service providers.
Finland
Main article: Healthcare in Finland
In Finland, public medical services at clinics and hospitals are run by the municipalities (local government) and are funded 76% by taxation, 20% by patients through access charges, and 4% by others. Private provision is mainly in the primary care sector. There are a few private hospitals.[81] The main hospitals are either municipally owned (funded from local taxes) or run by the medical teaching universities (funded jointly by the municipalities and the national government). According to a survey published by the European Commission in 2000, Finland's is in the top 4 of EU countries in terms of satisfaction with their hospital care system: 88% of Finnish respondents were satisfied compared with the EU average of 41.3%.[82] Finnish health care expenditures are below the European average.[83] The private medical sector accounts for about 14 percent of total health care spending. Only 8% of doctors choose to work in private practice, and some of these also choose to do some work in the public sector.[citation needed]
Taxation funding is partly local and partly nationally based. The national social insurance institution KELA reimburses part of patients prescription costs and makes a contribution towards private medical costs (including dentistry) if they choose to be treated in the private sector rather than the public sector. Patient access charges are subject to annual caps. For example, GP visits cost €11 per visit with annual €33 cap; hospital outpatient treatment €22 per visit; a hospital stay, including food, medical care and medicines €26 per 24 hours, or €12 if in a psychiatric hospital. After a patient has spent €683 per year on public medical services, all further treatment in that year is covered (although the required initial deductible is reviewed annually, so it may vary). There is a separate reimbursement system for prescribed medicine: after paying €578 per year, the remaining bought medicine will have a maximum price of €2.50 per purchase.[84]
Finland has a highly decentralized three-level public system of health care and alongside this, a much smaller private health care system.[85] Overall, the municipalities (funded by taxation, local and national) meet about two thirds of all medical care costs, with the remaining one third paid by the national insurance system (nationally funded), and by private finance (either employer-funded or met by patients themselves).[85] Private inpatient care forms about 3–4% of all inpatient care.[85] In 1999 only 17 per cent of total funding for health care came from insurance, comprising 14.9% statutory (government) insurance and 2.1% private health insurance. Eyeglasses are not publicly subsidized at all, although dentistry is available as a municipal service or can be obtained privately with partial reimbursement from the state.[85]
The percentage of total health expenditure financed by taxation in Finland (78%)[86] is above the OECD average and similar to the levels seen in Germany (77%) and France (80%) but below the level seen in the UK (87%). The quality of service in Finnish health care, as measured by patient satisfaction, is excellent. According to a survey published by the European Commission in 2000, Finland has one of the highest ratings of patient satisfaction with their hospital care system in the EU: 88% of Finnish respondents were satisfied compared with the EU average of 41.3%.[87]
There are caps on total medical expenses that are met out-of-pocket for drugs and hospital treatments. The National Insurance system pays all necessary costs over these caps. Public spending on health care in 2006 was 13.6 billion euros (equivalent to US$338 per person per month). The increase over 2005 at 8.2 per cent was below the OECD average of 9 percent. Household budgets directly met 18.7 per cent of all health care costs.[88]
France
Main article: Health care in France
France has a system of health care largely financed by government through a system of national health insurance. Nonetheless, not all medical care is paid for by the state, with only 70% of initial GP care covered and anywhere between 35% and 100% of prescription medication covered. It is consistently ranked as one of the best in the world.[89]
Georgia
Main article: Healthcare in Georgia (country)
In 2013, Georgia adopted a universal health care system. Healthcare in Georgia is provided by a universal health care system under which the state funds medical treatment in a mainly privatized system of medical facilities. In 2013, the enactment of a universal health care program triggered universal coverage of government-sponsored medical care of the population and improving access to health care services. Responsibility for purchasing publicly financed health services lies with the Social Service Agency (SSA).[90][91] However, according to the UN, due to the high out-of-pocket costs that patients incur, Georgia has not yet achieved universal healthcare.[92]
Germany
Main article: Health care in Germany
The Charité (Hospital) in Berlin
Germany has the world's oldest national social health insurance system,[93][94][95] with origins dating back to Otto von Bismarck's Sickness Insurance Law of 1883.[96][97] The system is decentralized with private practice physicians providing ambulatory care, and independent, mostly non-profit hospitals providing the majority of inpatient care. Employers pay for half of their employees' health insurance contributions, while self-employed workers pay the entire contribution themselves.[98] Approximately 90% of the population is covered by a statutory health insurance plan, which provides a standardized level of coverage through any one of approximately 100 public sickness funds.[98][99] The rest are covered by private health insurance. Private health insurance is only accessible to self-employed workers, high-income employees and Beamte. The contributions for public insurance is determined according to income, while the contributions for private health insurance are determined according to age and health condition.[98]
Purchasing basic health insurance is mandatory for all persons residing in Germany if not employed. Historically, the level of provider reimbursement for specific services is determined through negotiations between regional physician's associations and sickness funds. Since 1976 the government has convened an annual commission, composed of representatives of business, labor, physicians, hospitals, and insurance and pharmaceutical industries.[100] The commission takes into account government policies and makes recommendations to regional associations with respect to overall expenditure targets. In 1986 expenditure caps were implemented and were tied to the age of the local population as well as the overall wage increases. Although reimbursement of providers is on a fee-for-service basis, the amount to be reimbursed for each service is determined retrospectively to ensure that spending targets are not exceeded. Capitated care, such as that provided by U.S. health maintenance organizations, has been considered as a cost containment mechanism but would require consent of regional medical associations, and has not materialized.[101]
Copayments were introduced in the 1980s in an attempt to prevent overutilization and control costs. The average length of hospital stay in Germany has decreased in recent years from 14 days to 9 days, still considerably longer than average stays in the U.S. (5 to 6 days).[102][103] The difference is partly driven by the fact that hospital reimbursement is chiefly a function of the number of hospital days as opposed to procedures or the patient's diagnosis. Drug costs have increased substantially, rising nearly 60% from 1991 through 2005. Despite attempts to contain costs, overall health care expenditures rose to 10.7% of GDP in 2005, comparable to other western European nations, but substantially less than that spent in the U.S. (nearly 16% of GDP).[104]
Greece
Main article: Healthcare in Greece
The Greek healthcare system provides high quality medical services to insured citizens and is coordinated by the Ministry for Health and Social Solidarity. Public health services are provided by the National Healthcare Service, or ESY (Greek: Εθνικό Σύστημα Υγείας, ΕΣΥ). In 2010 there were 35,000 hospital beds and 131 hospitals in the country.
The Greek healthcare system has received high rankings by the World Health Organization, ranked 14th in the overall assessment and 11th in quality of service in a 2000 report by the WHO. However, it must be noted that the entire financial system collapsed in 2007–2008. The data listed above is from 2000.
Iceland
Main article: Healthcare in Iceland
Iceland has a universal public health system paid largely from taxation with local municipalities delivering health care services in the same way as the Scandinavian countries. Iceland's entire population has equal access to health care services.[citation needed][105]
Ireland
Main article: Healthcare in the Republic of Ireland
The public health care system in Ireland is governed by the Health Act 2004,[106] which established a new body to be responsible for providing health and personal social services to everyone living in Ireland – the Health Service Executive. The new national health service came into being officially on January 1, 2005; however, the new structures are currently[when?] in the process of being established as the reform program continues[citation needed]. In addition to the public-sector, there is a large private health care market.
In Ireland, 37% of the population have a means-tested medical card that gives the holder access to tax-funded GP care and requires €2.00 for each prescription drug.[107] The standard charge for Irish and EU citizens who attend the A&E in hospitals is €100. This is free of charge if referred by a GP.[108] For all other residents who do not have a medical card, the average price for an appointment with a family doctor GP is €50 or €70 for an emergency appointment with a Caredoc GP.[109] Ireland is currently in the process of establishing a universal healthcare system based on compulsory private health insurance, with competition managed by the government. These reforms are known as Sláintecare and are scheduled to be completed by 2030.[110]
Italy
Main article: Healthcare in Italy
Italy has a public health care service for all the residents called "Servizio Sanitario Nazionale" or SSN (National Health Service). It is publicly run and funded mostly by taxation. Some services require variable co-pays, while other services (such as emergency medicine and a general doctor) are free. There is also a small parallel private health care system, especially in the field of dentistry and optometry.
Latvia
Main article: Healthcare in Latvia
Healthcare in Latvia is universal for citizens of Latvia. The healthcare system in Latvia operates as a universal program that is primarily funded through government taxation.[111] It bears similarities to the National Health Service (NHS) in UK and employs a purchaser-provider split (PPS). Following several reforms, a National Health Service (NHS) type system, known as Nacionālais veselības dienests (NVD) in Latvian, was established in 2011.[112]
The NVD controls the implementation of healthcare policies while the Ministry of Health develops policies and oversees the system. Healthcare services are available for free for citizens of Latvia. The country's Ministry of Health manages its healthcare system through a combination of social insurance institutional body, legislative healthcare provision financed by taxes and numerous public and private providers.[113]
Despite near-universal population coverage provided by the NVD established in 2011, there are challenges to equitable access with issues around geographical distribution of health professionals, user charges and long waiting lists. The publicly funded health benefits package is limited in scope and only covers a predetermined set of services.[114][115]
Lithuania
Main article: Healthcare in Lithuania
The public healthcare system in Lithuania ensures free healthcare for almost all its citizens. This state-funded healthcare is available to long-term residents and expats too.
Luxembourg
Main article: Healthcare in Luxembourg
Luxembourg provides universal health care coverage to all residents (Luxembourgers and foreigners) by the National Health Insurance (CNS - Caisse nationale de santé (French) or National Gesondheetskeess (Luxembourgish)). It is funded by mandatory contributions of employers and the workforce, and by government subsidies for insuring jobseekers, the poor, and for financing medical infrastructure. The nation also has mandatory public long-term care insurance.[116][117]
Netherlands
Main articles: Healthcare in the Netherlands and Economic_interventionism § Market-driven_medical_welfare_state
The Netherlands has a dual-level system. All primary and curative care (family doctors, hospitals, and clinics) is financed from private compulsory insurance. Long-term care for the elderly, the dying, the long-term mentally ill etc. is covered by social insurance funded by public spending. According to the WHO, the health care system in the Netherlands was 62% government-funded and 38% privately funded as of 2004.[57]
Insurance companies must offer a core universal insurance package for universal primary, curative care, including the cost of all prescription medicines. They must do this at a fixed price for all. People pay the same premium whether young or old, healthy or sick. It is illegal in The Netherlands for insurers to refuse an application for health insurance, to impose special conditions (e.g., exclusions, deductibles, co-pays etc.), or refuse to fund treatments that a doctor has determined are medically necessary. The system is 50% financed from payroll taxes paid by employers to a fund controlled by the Health regulator. The government contributes an additional 5% to the regulator's fund. The remaining 45% is collected as premiums paid by the insured directly to the insurance company. Some employers negotiate bulk deals with health insurers and some even pay the employees' premiums as an employment benefit. The regulator has sight of the claims made by policyholders and therefore can redistribute the funds its holds on the basis of relative claims made by policy holders. Thus insurers with high payouts receive more from the regulator than those with low payouts. Insurance companies have no incentive to deter high-cost individuals from taking insurance and are compensated if they have to pay out more than might be expected. Insurance companies compete with each other on price for the 45% direct premium part of the funding and try to negotiate deals with hospitals to keep costs low. The competition regulator is charged with checking for abuse of dominant market positions and the creation of cartels that act against consumer interests. An insurance regulator ensures that all basic policies have identical coverage rules so that no person is medically disadvantaged by his or her choice of insurer.
Hospitals in the Netherlands are also regulated and inspected but are mostly privately run and not-for-profit, as are many of the insurance companies. Patients can choose where they want to be treated, and have access to information on the internet about the performance and waiting times at each hospital. Patients dissatisfied with their insurer and choice of hospital can cancel at any time but must make a new agreement with another insurer.
Insurance companies can offer additional services at an extra cost over and above the universal system laid down by the regulator, e.g., for dental care. The standard monthly premium for health care paid by individual adults is about €100 per month. Persons with low incomes can get assistance from the government if they cannot afford these payments. Children under 18 are insured by the system at no additional cost to them or their families because the insurance company receives the cost of this from the regulator's fund. There is a fixed yearly deductible of €385 for each adult person, excluding first visits for diagnosis to general physicians.
Norway
Main article: Healthcare in Norway
Norway has a universal public health system paid largely from taxation in the same way as other Scandinavian countries. The Norwegian health care system is government-funded and heavily decentralized. The health care system in Norway is financed primarily through taxes levied by county councils and municipalities. Dental care is included for children until 18 years old, and is covered for adults for some ailments.[118]
Norway regularly comes top or close to the top of worldwide healthcare rankings.
North Macedonia
Main article: Health in North Macedonia
The country inherited a large health infrastructure after independence in 1991 with good well-distributed public health services. Private hospitals were opened and primary care was privatised. Subsequently, both public and private providers have been integrated into one social insurance-funded model managed by the Health Insurance Fund of North Macedonia. The public hospital sector is seen as inefficient and is unpopular with both patients and professional staff. 90% of the population is within 30 minutes of a health service.
Expenditure on healthcare was $851 per head in 2014, 6.5% of GDP.
According to the Euro health consumer index the Macedonian health system made the most remarkable advance of any country in the history of their Index, from 27th to 16th place in 2014, because by implementing a real-time e-Booking system they reduced waiting lists so significantly. From July 2013, any GP can make a booking at any specialist or heavy diagnostic equipment in the country in real-time while the patient is present. They rated Macedonia 16th in Europe in 2015.
The Doctor's Chamber of Macedonia complains that there is a discrepancy between the available funds and the quality of service expected, that facilities are not used efficiently, equipment is outdated and staff are not used effectively.
Portugal
Main article: Health in Portugal
Portugal's National Healthcare Service, known nationally as Serviço Nacional de Saúde (SNS), is a universal and free healthcare service provided nationwide since 1979 and available to both Portuguese and foreign residents. In 2014, Portugal SNS ranked 13th best healthcare service in Europe.[119] The National Medical Emergency Institute (INEM) is the main emergency medical service and can be activated by calling 112.
Romania
Main article: Healthcare in Romania
According to Article 34 of the Constitution of Romania, the state is obliged "to guarantee the protection of healthcare". Romania has a fully universal healthcare system, which covers medical check-ups, surgical interventions, and any postoperative medical care, as well as free or subsidized medicine for a range of diseases. The state is also obliged to fund public hospitals and clinics. Dental care is not funded by the state, although there are public dental clinics in some hospitals, which treat patients free of charge.
Russia
Main article: Healthcare in Russia
In the former Soviet Union, the preferred term was "socialist medicine"; the Russian language has no term to distinguish between "socialist" and "socialized" (other than "public", Rus: obshchestvenniy/общественный, sometimes "collectivized" or "nationalized", Rus: obobshchestvlenniy/обобществленный).[120][121]
Russia in Soviet times (between 1917 and 1991) had a totally socialist model of health care with a centralized, integrated, hierarchically organised government providing free health care to all citizens. Quality of care and access to medications was not equal however and was dependent on the social status of patient. The best care was provided for nomenklatura and their family members, who had been segregated from the rest of population facilities, such as Kremlin hospital.[122] Initially successful at combating infectious diseases, the effectiveness of the socialized model declined with underinvestment. Despite a doubling in the number of hospital beds and doctors per capita between 1950 and 1980, the quality of care began to decline by the early 1980s and medical care and health outcomes were below western standards.
The new mixed economy Russia has switched to a mixed model of health care with private financing and provision running alongside state financing and provision. The OECD reported that unfortunately, none of this has worked out as planned and the reforms have in many respects made the system worse.[123][needs update] The population's health has deteriorated on virtually every measure. The resulting system is overly complex and very inefficient. It has little in common with the model envisaged by the reformers. Although there are more than 300 private insurers and numerous public ones in the market, real competition for patients is rare leaving most patients with little or no effective choice of insurer, and in many places, no choice of health care provider either. The insurance companies have failed to develop as active, informed purchasers of health care services. Most are passive intermediaries, making money by simply channelling funds from regional OMS funds to healthcare providers.
Article 41 of the Constitution of the Russian Federation confirms a citizen's right to state healthcare and medical assistance free of charge.[124] This is achieved through state compulsory medical insurance (OMS), which is funded by an obligatory medical insurance payroll tax and government subsidies.[125][126] It is worth mentioning that Russian citizens never pay taxes for themselves and often don't even know how much taxes they pay, because tax payment process is maintained by companies they are working on.[127] Introduction in 1993 reform of new free market providers in addition to the state-run institutions intended to promote both efficiency and patient choice. A purchaser-provider split helps facilitate the restructuring of care, as resources would migrate to where there was greatest demand, reduce the excess capacity in the hospital sector and stimulate the development of primary care. Russian Prime Minister Vladimir Putin announced a new large-scale health care reform in 2011 and pledged to allocate more than 300 billion rubles ($10 billion) in the next few years to improve health care in the country. As of 2020 the health insurance tax (called deposition to an OMS fund) is 5.1%.[128]
Serbia
Main article: Healthcare in Serbia
The Constitution of the Republic of Serbia states that it is the right of every citizen to seek medical assistance free of charge.[129] This is achieved by mutual contribution to the Compulsory Social Healthcare Fund of RZZO (Republički Zavod za Zdravstveno Osiguranje or National Health Insurance Institution). The amount of contribution depends on the amount of money the person is making.
Spain
Main article: Healthcare in Spain
Spain provides a public universal health care system for all citizens and, under certain conditions, also non-citizens. Healthcare is free except for co-payments for some products and services; it is mostly paid from the Social Security budget. Adult dental care is not covered but for basic extractions or problems that could result in serious stomatological conditions.
Irrespective of the nationality and insurance situation of the patient, the public system always treats medical emergencies until achieving the best possible outcome. If not covered by the Spanish Social Security (i.e., a visiting foreigner), the provider later negotiates payment with the patient or the patient's insurer. If actually unable to pay, it is covered by Social Security on humanitarian grounds unless the patient purposely traveled to Spain to get free healthcare. Obvious unexpected emergencies such as accidental injuries or sudden illness are customarily covered, but those that could be reasonably expected (e.g., arising from a chronic condition or from avoidable risk-taking) are studied on a case-per-case basis.
According to the World Economic Forum and to Bloomberg, Spain has the most efficient health system in Europe, and also ranks at the top worldwide along with Hong Kong, Japan and Singapore.[130][131]
Private health insurance is available for those who prefer it, and recommended for visitors not covered by the Spanish Social Security or a foreign public or private insurer with overseas coverage.
Sweden
Main article: Healthcare in Sweden
Sweden has a universal public health care system paid for through taxation. The Swedish public and private health care systems are funded through taxes levied by the county councils. Government-paid dental care is accessible to those under 23 years old.
Sweden also has a smaller private health care sector, mainly in larger cities or as centers for preventive health care financed by employers.
In recent years the health care system of Sweden has been heavily criticized for not providing the same quality of health care to all Swedish citizens.[132][133][134][135] This was especially brought to light during the COVID-19 pandemic as Swedish media and public health researchers pointed out that Swedish citizens of other ethnicities than Swedish and people living in working class areas were dying from COVID-19 at a significantly higher rate than the rest of the population.[136][137][138]
Switzerland
Main article: Healthcare in Switzerland
Purchasing basic health insurance is mandatory for all persons residing in Switzerland (within three months of taking up residence or being born in the country).[139] Healthcare in Switzerland is universally available and is regulated by the Federal Health Insurance Act of 1994. Supplemental insurance plans are optional. Insurers are required to offer insurance to everyone, regardless of age or medical condition. They are not allowed to make a profit off this basic insurance, but can on supplemental plans.[140]
Turkey
Main article: Healthcare in Turkey
Turkey achieved universal health coverage in 2003.[141]
The Government's Health Transformation Program of 2003 established a common benefit package that covers primary and preventive care, ambulatory and inpatient care, laboratory services, rehabilitation and follow-up services, pharmaceuticals and medical aids and appliances.[141] Payroll taxes of 12.5% of a person's gross income (5% by the employee and 7.5% by the employer) fund 97%[142] of the program. The government provides for the remaining 3% of the cost.[143]
United Kingdom
Main article: Healthcare in the United Kingdom
Each of the countries of the United Kingdom has a National Health Service that provides public healthcare to all UK permanent residents that was originally designed to be free at the point of need and paid for from general taxation; but changes included introducing charging for prescription medicines and dentistry (those below 16 and those on certain benefits may still get free treatment). However, since health is now a devolved matter, considerable differences are developing between the systems in each of the countries for example Northern Ireland, Scotland and Wales abolished prescription charges.[144] Private healthcare companies are free to operate alongside the public system.
England
Main article: Healthcare in England
Norfolk and Norwich University Hospital, a National Health Service hospital.
The National Health Service (NHS), created by the National Health Service Act 1946, has provided the majority of healthcare in England since its launch on July 5, 1948.[citation needed]
The NHS Constitution for England documents, at a high level, the objectives of the NHS, the legal rights and responsibilities of the various parties (patients, staff, NHS trust boards), and the guiding principles that govern the service.[145] The NHS constitution makes it clear that it provides a comprehensive service, available to all irrespective of age, gender, disability, race, sexual orientation, religion, or belief; that access to NHS services is based on clinical need and not an individual's ability to pay; and that care is never refused on unreasonable grounds. Patient choice in terms of doctor, care, treatments, and place of treatment is an important aspect of the NHS's ambition, and in some cases patients can elect for treatment in other European countries at the NHS's expense. Waiting times are low, with most people able to see their primary care doctor on the same day or the following day.[146] Only 36.1% of hospital admissions are from a waiting list, with the remainder being either emergencies admitted immediately or else pre-booked admissions or the like (e.g., child birth).[147] One of the main goals of care management is to ensure that patients do not experience a delay of more than 18 weeks from initial hospital referral to final treatment, inclusive of time for all associated investigative tests and consultations.[148] In 2009, two-thirds of patients were treated in under 12 weeks.[149]
Though centrally funded, the NHS is not managed by a large central bureaucracy. Responsibility is divided among geographical areas through strategic health authorities. Management is distributed even more locally through primary care trusts, hospital trusts—and increasingly to NHS foundation trusts that provide even more decentralized services within the NHS framework, with more decisions left to local people, patients, and staff. The central government office—the Department of Health—is not involved in day-to-day decision making in either the Strategic Health Authorities or the individual local trusts (primarily health, hospital, or ambulance) or the national specialist trusts such as NHS Blood and Transplant. It does lay down general guidelines they must follow. Local trusts are accountable to their local populations, whilst government ministers are accountable to Parliament for the service overall.[citation needed]
The NHS provides, among other things, primary care, in-patient care, long-term healthcare, psychiatric care and treatments, ophthalmology, and dentistry. All treatment is taxpayer-funded with the exception of certain charges for prescriptions, dentistry and ophthalmology (which themselves are free to children, certain students in full-time education, the elderly, the unemployed and those on low incomes). Around 89 percent of NHS prescriptions are obtained free of charge, mostly for children, pensioners, and pregnant women. Others pay a flat rate of £9.00, and others may cap their annual charges by purchasing an NHS Prescription Prepayment Certificate. Private health care has continued parallel to the NHS, paid for largely by private insurance. Private insurance accounts for only 4 percent of health expenditure and covers little more than a tenth of the population.[150] Private insurers in the UK only cover acute care from specialists. They do not cover generalist consultations, pre-existing conditions, medical emergencies, organ transplants, chronic conditions such as diabetes, or conditions such as pregnancy or HIV.[151]
Most NHS general practitioners are private doctors who contract to provide NHS services, but most hospitals are publicly owned and run through NHS trusts. A few NHS medical services (such as "surgicentres") are sub-contracted to private providers[152] as are some non-medical services (such as catering). Some capital projects such as new hospitals have been funded through the Private Finance Initiative, enabling investment without (in the short term) increasing the public sector borrowing requirement, because long-term contractually obligated PFI spending commitments are not counted as government liabilities.[citation needed]
Northern Ireland
Main article: Health and Social Care in Northern Ireland
Health and Social Care in Northern Ireland is the designation of the national public health service in Northern Ireland.
Scotland
Main article: Healthcare in Scotland
The Royal Aberdeen Children's Hospital is a specialist children's hospital within NHS Scotland.
NHS Scotland, created by the National Health Service (Scotland) Act 1947, was also launched on July 5, 1948, although it has always been a separate organization. Since devolution, NHS Scotland has followed the policies and priorities of the Scottish Government, including the phasing out of all prescription charges by 2011. Prescriptions are now free in Scotland for all citizens. All healthcare in Scotland remains free at the point of use.
Wales
Main article: Healthcare in Wales
NHS Wales was originally formed as part of the same NHS structure created by the National Health Service Act 1946 but powers over the NHS in Wales came under the Secretary of State for Wales in 1969,[153] in turn being transferred under devolution to what is now the Welsh Government.
Crown dependencies
Isle of Man
The Isle of Man, a UK Crown dependency, provides universal public health coverage to its residents.[154]
Guernsey/Jersey
The medical care system in the Channel Islands is very similar to that of the UK in that many of the doctors and nurses have been trained from the UK health perspective.
There is universal health care for residents of Jersey.[155]
Healthcare in Guernsey and Alderney is charged for[156] with all primary care provided for on a private basis.[157][158]
There is no universal healthcare for residents of Sark.
North America
The Bahamas, Barbados, Canada, Costa Rica, Cuba, Jamaica, Mexico, Panama, and Trinidad and Tobago all provide some level of universal health coverage.
Bahamas
The Bahamas approved the National Health Insurance Act in August 2016. The legislation establishes a universal health coverage system that begins with universal coverage of primary health care services, and later expands to include a wide set of benefits that includes all specialized care. The system allows for universal coverage of a basic benefits package and for voluntary insurance to be purchased as a top-up policy to cover services or amenities that are not included in the government plan.[159]
Canada
Main article: Health care in Canada
In 1984, the Canada Health Act was passed, which prohibited extra billing by doctors on patients while at the same time billing the public insurance system. In 1999, the prime minister and most premiers reaffirmed in the Social Union Framework Agreement that they are committed to health care that has "comprehensiveness, universality, portability, public administration and accessibility."[160]
The system is for the most part publicly funded, yet most of the services are provided by private enterprises or private corporations,[citation needed] although most hospitals are public. Most doctors do not receive an annual salary, but receive a fee per visit or service.[161] About 29% of Canadians' health care is paid for by the private sector or individuals.[162] This mostly goes towards services not covered or only partially covered by Medicare such as prescription drugs, dentistry, physiotherapy and vision care.[163] Many Canadians have private health insurance, often through their employers, that cover these expenses.[164]
The Canada Health Act of 1984 "does not directly bar private delivery or private insurance for publicly insured services," but provides financial disincentives for doing so. "Although there are laws prohibiting or curtailing private health care in some provinces, they can be changed," according to a report in the New England Journal of Medicine.[165][166] The legality of the ban was considered in a decision of the Supreme Court of Canada, which ruled in Chaoulli v. Quebec that "the prohibition on obtaining private health insurance, while it might be constitutional in circumstances where health care services are reasonable as to both quality and timeliness, is not constitutional where the public system fails to deliver reasonable services." The appellant contended that waiting times in Quebec violated a right to life and security in the Quebec Charter of Human Rights and Freedoms. The Court agreed, but acknowledged the importance and validity of the Canada Health Act, and at least four of the seven judges explicitly recognized the right of governments to enact laws and policies that favour the public over the private system and preserve the integrity of the public system.
Costa Rica
Universal healthcare and pensions are run by the Caja Costarricense de Seguro Social (CCSS). In 1941, Costa Rica established Caja Costarricense de Seguro Social (CCSS), a social security insurance system for wage-earning workers. In 1961, coverage was expanded to include workers' dependents and from 1961 to 1975, a series of expansions extended coverage for primary care and outpatient and inpatient specialized services to people in rural areas, the low-income population, and certain vulnerable populations. Further expansions during the late 1970s extended insurance coverage to farmers, peasants, and independent contract workers. Additionally, CCSS mandates free health service provision to mothers, children, indigenous people, the elderly, and people living with disabilities, regardless of insurance coverage. By 2000, 82 percent of the population was eligible for CCSS, which has continued to expand in the ensuing period. By covering all population groups through the same system, Costa Rica has avoided social insurance stratification and inequity common in many other countries in the region.[167]
CCSS is funded by a 15 percent payroll tax, as well as payments from retiree pensions [6]. Taxes on luxury goods, alcohol, soda, and imported products also help to cover poor households who do otherwise pay into the system. All CCSS funds are merged into a single pool, which is managed by the central financial administration of CCSS. In 1973, the Ministry of Health decided to move away from direct service provision and adopt a steering role. Responsibility for the provision of most care was transferred to the CCSS, although the Ministry retained responsibility for disease control, food and drug regulation, environmental sanitation, child nutrition, and primary care for the poor. Through the CCSS, health care is now essentially free to nearly all Costa Ricans. Private health care is also widely available and INS offers private health insurance plans to supplement CCSS insurance.[168]
Cuba
Main article: Healthcare in Cuba
The Cuban government operates a national health system and assumes fiscal and administrative responsibility for the health care of all its citizens. There are no private hospitals or clinics as all health services are government-run. All healthcare in Cuba is free to Cuban residents.[169] The present Minister for Public Health is Roberto Morales Ojeda. The Cuban government sends doctors and other medical personnel overseas as part of medical missions. These missions are mainly in Latin America, Africa, and Oceania and have had substantial positive impacts on the local populations served. Cuba also brings medical students and patients to Cuba for training and treatment respectively.
Mexico
Main article: Healthcare in Mexico
Public health care became universal healthcare on January 1, 2020,[170] mandated by the new President Andrés Manuel López Obrador and approved by Congress. It is completely free for Mexican citizens who do not have health insurance. Mexico's new universal healthcare, administered by the Instituto de Salud para el Bienestar (Institute of Health for Welfare, INSABI), includes free consultations with family doctors and specialists, free medications, free surgeries, free dental and vision[citation needed]. As of 2020, public health care is provided to all Mexican citizens as guaranteed via Article 4 of the Constitution. Public care is now fully subsidized by the federal government. All Mexican citizens are eligible for subsidized health care regardless of their work status via a system of health care facilities operating under the federal Secretariat of Health (formerly the Secretaria de Salubridad y Asistencia, or SSA) agency.
Employed citizens and their dependents, however, are further eligible to use the health care program administered and operated by the Instituto Mexicano del Seguro Social (IMSS) (English: Mexican Social Security Institute). The IMSS health care program is a tripartite system funded equally by the employee, its private employer, and the federal government. The IMSS does not provide service to employees of the public sector. Employees in the public sector are serviced by the Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado (ISSSTE) (English: Institute for Social Security and Services for State Workers), which attends to the health and social care needs of government employees. This includes local, state, and federal government employees. The government of the states in Mexico also provide health services independently of those services provided by the federal government programs. In most states, the state government has established free or subsidized healthcare for all their citizens.
In 2006, the Mexican government created the Health Insurance for a New Generation also known as "life insurance for babies".[171][172][173] On May 28, 2009, Universal Care Coverage for Pregnant Women was introduced.[174] In a 2020 expansion of health care coverage, all Mexicans are now covered.
Trinidad and Tobago
Main article: Healthcare in Trinidad and Tobago
A universal health care system is used in Trinidad and Tobago and is the primary form of health care available in the country. It is used by the majority of the population seeking medical assistance, as it is free for all citizens. Responsibility for the provision of healthcare services in Trinidad and Tobago was devolved from the Ministry of Health to Regional Health Authorities under the Regional Health Authorities Act No. 5 in 1994.
United States
Main article: Healthcare in the United States
Between 2010 and 2019, the individual shared responsibility provision of the Affordable Care Act required Americans, with certain exemptions, to have private or public health insurance.[175] Otherwise, they were required to pay a fine.
South America
Argentina, Brazil, Chile, Colombia, Ecuador, Peru, Uruguay, and Venezuela all provide some level of universal health coverage.
Argentina
Main article: Health care in Argentina
Health care is provided through a combination of employer and labor union-sponsored plans (Obras Sociales), government insurance plans, public hospitals and clinics and through private health insurance plans. It costs almost 10% of GDP and is available to anyone regardless of ideology, beliefs, race or nationality.
Brazil
Main article: Healthcare in Brazil
The universal health care system was adopted in Brazil in 1988 after the end of the military dictatorship. However, universal health care was available many years before, in some cities, once the 27th amendment to the 1969 Constitution imposed the duty of applying 6% of their income in healthcare on the municipalities.[176] The Brazilian universal health care is called SUS (Sistema Único de Saúde), which covers all treatments, surgeries and medications for all resident and non-resident individuals within Brazilian jurisdiction, regardless of ethnicity, nationality, or visa - including tourists, passengers in transit and refugees.
Chile
Main article: Healthcare in Chile
Health care in Chile is provided by the government (via public corporation FONASA, National Healthcare Fund) and by private insurers (via ISAPRE, Previsional Healthcare Institutions). All workers and pensioners are mandated to pay 7% of their income for health care insurance (the poorest pensioners are exempt from this payment but medications are expensive and pensioners have to pay). Workers who choose not to join an Isapre, are automatically covered by Fonasa. Fonasa also covers unemployed people receiving unemployment benefits, uninsured pregnant women, insured worker's dependant family, people with mental or physical disabilities and people who are considered poor or indigent.
Fonasa costs vary depending on income, disability or age. Attention at public health facilities via Fonasa is free for low-income earners, people with mental or physical disabilities and people over the age of 60. Others pay 10% or 20% of the costs, depending on income and the number of dependants. Fonasa beneficiaries may also seek attention in the private sector, for a designated fee.
Additionally, exist the GES Plan (Explicit Guarantees in Healthcare Plan), that consists of a defined number of high-morbility and mortality diseases (currently 85) that have special mandatory attention guarantees for all people, both Isapre and Fonasa affiliates, in relation to:
Access: Universal access to treatment if required. Individuals will be able to get attention from a provider near their place of residence.
Opportunity: Opportune waiting times, there is a maximum pre-established time limit to get initial and post-diagnosis attention.
Financial protection: Law-fixed maximum price with low copayments to providers (maximum copayment of 20% of the cost), the payment cannot be an obstacle to attention. The total cost must not exceed one monthly income for the family in a year.
Best possible quality of service: Attention only in accredited public or private Health centers, that follow technical requirement standards that will be established based on medical evidence.
The treatment protocols and number of diseases included are evaluated every 3 years by the authorities.
Colombia
Main article: Health care in Colombia
In 1993 a reform transformed the health care system in Colombia, trying to provide a better, sustainable, health care system and to reach every Colombian citizen.
Peru
Main article: Healthcare in Peru
On April 10, 2009, the Government of Peru published the Law on Health Insurance to enable all Peruvians to access quality health services, and contribute to regulating the financing and supervision of these services. The law enables all population to access diverse health services to prevent illnesses, and promote and rehabilitate people, under a Health Basic Plan (PEAS).[177][178]
On April 2, 2010, President Alan Garcia Perez signed a supreme ordinance approving the regulations for the framework law on Universal Health Insurance, which seeks to provide access to quality health care for all Peruvian citizens.
Peru's Universal Health Insurance law aims to increase access to timely and quality health care services, emphasizes maternal and child health promotion, and provides the poor with protection from financial ruin due to illness.[179]
The regulation states that membership of the Universal Health Insurance (AUS for its Spanish acronym) is compulsory for the entire population living in the country. To that end, the Ministry of Health will approve, by supreme ordinance, the mechanisms leading to compulsory membership, as well as escalation and implementation.[180]
Suriname
Main article: Health in Suriname
The National Basic Health Insurance Law, introduced in 2014, provides access to a basic package of primary, secondary, and tertiary care services for citizens. It repeals the Healthcare Tariffs Law from 2005.
Uruguay
Main article: Health in Uruguay
Public health insurance is available, but not mandatory, to all residents.
Oceania
Australia and New Zealand both have universal health care. Hospitalisation is free for permanent residents in both nations. In addition, Australia grants primary care coverage, while in New Zealand general practice and prescriptions are subsidised only.
Australia
Main articles: Medicare (Australia) and Health care in Australia
In Australia, Medibank—as it was then known—was introduced, by the Whitlam Labor government on July 1, 1975, through the Health Insurance Act 1973. The Australian Senate rejected the changes multiple times and they were passed only after a joint sitting after the 1974 double dissolution election. However, Medibank was supported by the subsequent Fraser Coalition (Australia) government and became a key feature of Australia's public policy landscape. The exact structure of Medibank/Medicare, in terms of the size of the rebate to doctors and hospitals and the way it has administered, has varied over the years. The original Medibank program proposed a 1.35% levy (with low-income exemptions) but these bills were rejected by the Senate, so Medibank was funded from general taxation. In 1976, the Fraser Government introduced a 2.5% levy and split Medibank in two: a universal scheme called Medibank Public and a government-owned private health insurance company, Medibank Private.
In 1984, Medibank Public was renamed Medicare by the Hawke Labor government, which also changed the funding model, to an income tax surcharge, known as the Medicare Levy, which was set at 1.5%, with exemptions for low-income earners.[181] The Howard Coalition government introduced an additional levy of 1.0%, known as the Medicare Levy Surcharge, for those on high annual incomes ($70,000) who do not have adequate levels of private hospital coverage.[182] This was part of an effort by the Coalition to encourage take-up of private health insurance. According to WHO, government funding covered 67.5% of Australia's health care expenditures in 2004; private sources covered the remaining 32.5% of expenditures.[57]
As of 2019, the Medicare levy is 2% of taxable income,[183] with a Medicare levy surcharge, for those on high income who do not have appropriate private patient hospital cover (1% for singles on $90,000 pa and families on $180,000 pa, rising to 1.5% for higher incomes).[184]
In addition to Medicare, there is a separate Pharmaceutical Benefits Scheme, funded by the federal government, which substantially subsidises a range of prescription medications.
New Zealand
Main article: Health care in New Zealand
As with Australia, New Zealand's healthcare system is funded through general taxation according to the Social Security Act 1938. However, aside from hospitalisation, there are user charges for prescriptions (introduced in February 1985, (this ended in mid 2023 when funded drugs became free under prescription)) and partial subsidisation of general practitioner visits with additional provision for those on low or modest incomes known as Community Service Cards (introduced on February 1, 1992) to target healthcare based on income.[185][186][187] These changes were part of broader controversial policies introduced by the Fourth National Government between 1991 and 1993 and effectively ended largely free provision of primary healthcare. According to the WHO, government sources covered 77.4% of New Zealand's health care costs in 2004; private expenditures covered the remaining 22.6%.
Historic attempts to bring general practitioner care into government ownership have been largely unfulfilled.
There are twenty district health boards as of 2019 whose task is ensuring the provision of health and disability services to populations within a defined geographical area and are partially elected while the remainder is appointed by New Zealand's Minister of Health.[188] This system of management came into being on January 1, 2001, abolishing the much controversial Crown Health Enterprises regime which had replaced Area Health Boards previously.
https://en.wikipedia.org/wiki/List_of_c ... ealth_care
Y lo realmente embriagador para Trump es saber lo fácil que fue convencer a la base republicana de que sus mentiras eran la verdad del evangelio.
-
verdinegro
- Mensajes: 15294
- Registrado: Sab Dic 18, 2021 10:30 am
- Ubicación: Evropa
- Contactar:
Re: Texit: ¿Es posible la secesión de Texas?
No es poca cosa lo que está pasando en EE.UU. Es una rebelión abierta de los estados que se han ofrecido enviar a la Guardia Nacional para resguardar la frontera en Texas. También hay apoyo de las milicias. No la tiene nada fácil Biden... Esto se pudo evitar si la Corte Suprema no hubiese fallado en contra de Texas. El presidente de la Corte Suprema es un traidor.